

Using the ABN Tutorial
Select any field (letters A–J) for details on how to complete each ABN section.
Quick Start
The Advance Beneficiary Notice of Non-coverage (ABN), Form (CMS-R-131) helps Medicare Fee-for-Service (FFS) patients make informed decisions about items and services Medicare usually covers but may not in specific situations. For example, the items or services may not be medically necessary for a patient.
When health care providers and suppliers expect a Medicare coverage denial for a service we generally cover, they must issue an ABN to transfer the financial liability to the patient, including:
- Independent labs, skilled nursing facilities, and home health agencies providing Medicare Part B (outpatient) items and services
- Hospice providers, home health agencies, and religious non-medical health care institutions providing Part A (inpatient) items and services
This educational tool shows health care providers and suppliers how to correctly complete an ABN form. In this ABN tutorial, you refers to the provider or supplier issuing the form, while on the ABN form, you refers to the patient signing it.

Requirements
You must issue an ABN:
- When a Medicare item or service isn’t reasonable and necessary under Program standards, including care that’s:
- Not indicated for the diagnosis, treatment of illness, injury, or to improve the functioning of a malformed body member
- Experimental and investigational or considered research only
- More than the number of services allowed in a specific period for that diagnosis
- When providing custodial care
- When outpatient therapy services aren’t medically reasonable and necessary
Note: You must use the appropriate modifiers (for example, apply the KX modifier to the claim to indicate therapy above the thresholds is medically reasonable and necessary) - Before caring for a patient who isn’t terminally ill (hospice providers)
- Before caring for a patient who isn’t confined to the home or doesn’t need intermittent skilled nursing care (home health providers)
- Before providing a preventive service we usually cover but won’t cover in specific situations when services exceed frequency limits
- Before providing a Medicare item or service we won’t cover (DMEPOS suppliers) because the:
- Provider accepted prohibited unsolicited phone contacts
- Supplier hasn’t met supplier number requirements
- Non-contract supplier provides an item listed in a competitive bidding area
- Patient wants the item or service before the advance coverage determination
We may hold you financially liable if you don’t give the patient an ABN in these situations.
Don’t use an ABN for Medicare Advantage (Part C) or Medicare Prescription Drug Benefit (Part D) items and services.
You don’t need to notify the patient before you provide items or services that aren’t a benefit or never covered. Section 20.2 of the Medicare Claims Processing Manual, Chapter 30 has a list of items and services Medicare doesn’t cover.
We recommend issuing a voluntary ABN or a similar notice as a courtesy to alert the patient about their financial liability.
An ABN is valid if you:
- Use the most recent version approved by the Office of Management and Budget (OMB)
- Complete the entire form
- Ensure the patient understands the notice
An ABN remains effective after valid delivery if there’s no change in:
- Care from what’s described on the original ABN
- The individual’s health status which would require a change in the subsequent treatment for the non-covered condition
- The Medicare coverage guidelines for the items or services in question
What if the Patient or Their Representative Refuses to Choose an Option or Sign the ABN?
If the patient or their representative refuses to choose an option or sign the ABN, note the refusal on the original ABN. You can list refusal witnesses, but it’s not required. If a patient refuses to sign a properly issued ABN, consider not providing the item or service unless the consequences (health and safety of the patient or civil liability in case of harm) prevent it.
ABN Tutorial
In this tutorial, select any field (letters A–J) for details on how to complete each ABN section.
Entities who issue ABNs are collectively known as “notifiers,” which can include physicians, practitioners, providers (including labs) and suppliers, and utilization review committees.
If you reproduce the ABN, remove the letters before issuing it to the patient.
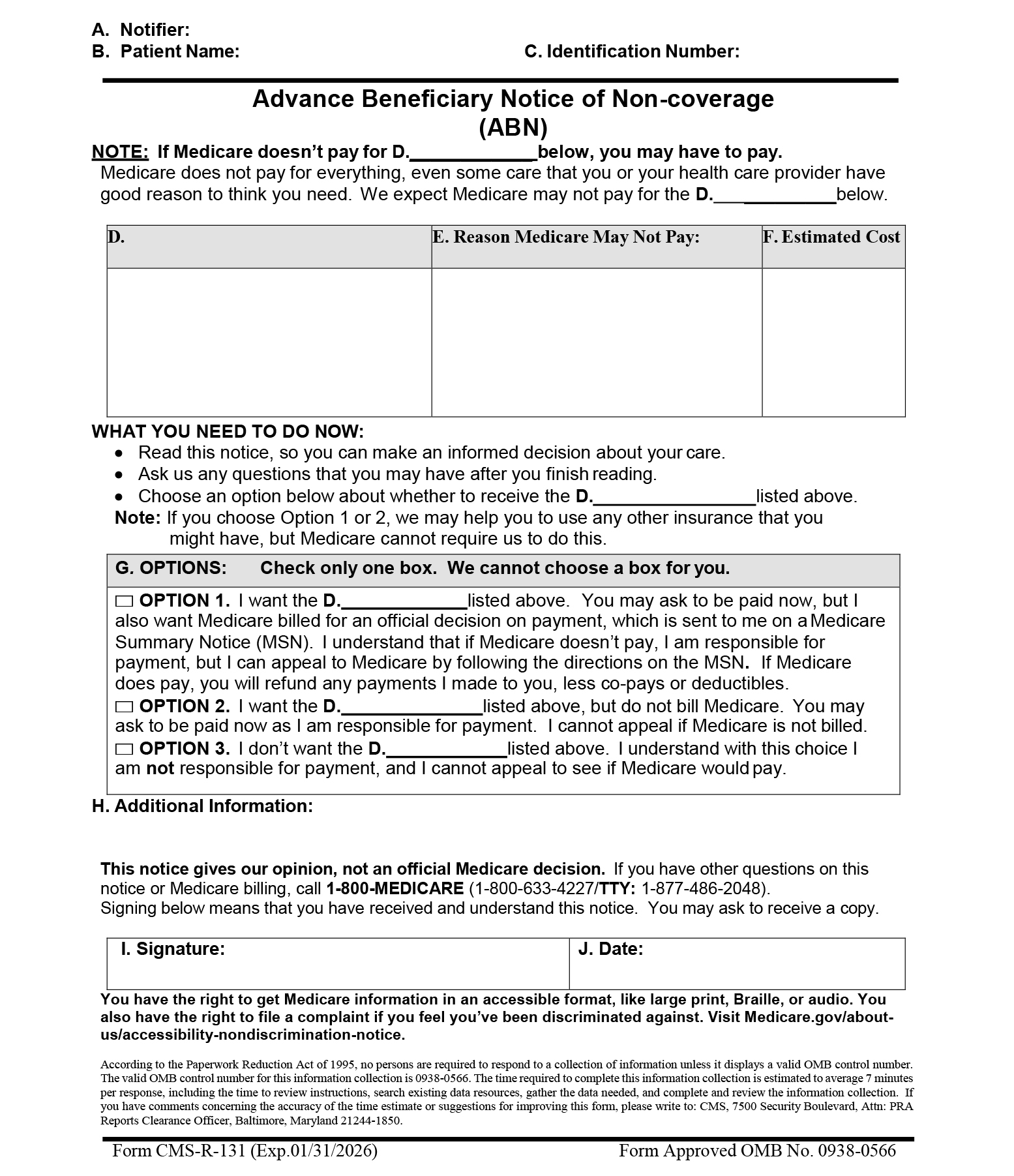
A. Notifier
- You must place the notifier’s name, address, and phone number (including TTY number, when needed) at the top of the notice. You can add this information to your logo at the top of the notice by typing, writing, pre-printing, using a label, or other means.
- If you and the billing entity aren’t the same, you can list more than 1 notifier if you specify in the Additional Information (H) section who we should contact with billing questions.
B. Patient Name
You must enter the patient’s first and last name and include a middle initial if it appears on their Medicare card. We won’t invalidate the ABN because of a misspelling or missing initial if the patient or representative recognizes the name listed on the notice as the patient’s.
C. Identification Number
This field is optional. Having no identification number doesn’t invalidate the ABN. You may enter a patient identification number that links the notice with a related claim, and you may create an internal filing number, like a medical record number. Don’t list MBIs or SSNs on the notice.
First ABN D. Field
List 1 of these descriptors:
- Item
- Service
- Lab test
- Test
- Procedure
- Care
- Equipment
Second ABN D. Field
Use the same wording used in the first (D) field.
Third ABN D. Field
Use the same wording used in the first (D) field.
First D. Column
- The notifier must list the specific items or services they believe we won’t cover in the blank (D) column.
- In a partial denial case, you must list the item’s or service’s excess components for which you expect denial in the blank (D) column.
- Put general descriptions of specifically grouped supplies in this column. For example, “wound care supplies” is enough to describe an item group. We generally don’t require an itemized list of each supply.
- When you reduce a service, you must provide enough information so the patient understands why. For example, we consider “wound care supplies decreased from weekly to monthly” enough to describe a frequency decrease for this supply category; just writing “wound care supplies decreased” isn’t enough.
- You must complete all 7 blank (D) fields to validate the notice. We encourage you to populate all blank (D) fields before using a general descriptor like “items or services.”
E. Reason Medicare May Not Pay
In this column, notifiers must explain, in patient-friendly language, why they believe we may not cover the items or services in column (D). We commonly use these non-coverage reasons:
- We don’t pay for this test for your condition
- We don’t pay for this test this often (denied as too frequent)
- We don’t pay for experimental or research tests
To be a valid ABN, you must list at least 1 reason for each item or service in column (D). You can use the same non-coverage reason for multiple items in column (D) when appropriate.
F. Estimated Cost
- Notifiers must complete column (F) to ensure the patient has all available information to decide whether to get potentially non-covered services.
- You must make a good faith effort to list a reasonable dollar estimate for all items or services in column (D). We expect the estimate be within $100 or 25% of actual costs, whichever is greater; generally, we accept estimates exceeding the actual cost since it won’t harm the patient if actual costs are less than predicted.
- Notifiers can bundle routinely grouped items or services into a single cost estimate. For example, you may give a single cost estimate for a group of lab tests, like a basic metabolic panel. We accept an average daily cost estimate for long-term or complex projections.
- You may also pre-print a menu of items or services in column (D) and include a cost estimate beside each item or service. If a situation calls for additional tests or procedures (like lab reflex testing), and you can’t reasonably estimate those test costs at the ABN delivery, you may enter the initial cost estimate and indicate possible further testing.
- If you can’t provide a good faith projected cost estimate at the ABN delivery, you may indicate in the cost estimate area that no cost estimate is available. You shouldn’t use these last 2 scenarios routinely, but the patient has the option of signing the ABN and accepting liability in these situations.
G. Options
Complete the 3 (D) fields under the (G) Options section with the same wording used in the first (D) field. The patient, or their representative, must choose 1 of the 3 options listed. We don’t allow you to make this selection.
Special guidance for people who are dually enrolled in both Medicare and Medicaid, also known as dually eligible individuals (has a Qualified Medicare Beneficiary (QMB) Program or Medicaid coverage), ONLY:
Instruct them to check ABN Option Box 1 so the notifier can submit the claim for Medicare adjudication. Strike through Option Box 1 language as shown here:
□ OPTION 1. I want the D._______ listed above. You may ask to be paid now, but I also want Medicare billed for an official decision on payment, which is sent to me on a Medicare Summary Notice (MSN). I understand that if Medicare doesn’t pay, I am responsible for payment, but I can appeal to Medicare by following the directions on the MSN.
If Medicare does pay, you will refund any payments I made to you, less co-pays or deductibles.
We require these edits because the notifier can’t bill the dually eligible patient when they offer an ABN. You can’t bill the patient pending Medicare and Medicaid adjudication because federal law affects dually eligible patient coverage and billing.
If we deny a claim when you needed an ABN to transfer financial liability to the patient, cross the claim over to Medicaid or submit it for adjudication based on state Medicaid coverage and payment policy. Medicaid will issue a remittance advice based on this determination. Once Medicare and Medicaid adjudicate the claim, you may only charge the patient in these circumstances:
- If the patient has QMB coverage without full Medicaid coverage, the ABN could allow you to shift financial liability to the patient per Medicare policy
- If the patient has full Medicaid coverage and Medicaid denies the claim (or won’t pay because you don’t participate in Medicaid), the ABN could allow you to shift financial liability to the patient per Medicare policy, subject to state laws that limit patient liability
Note: The patient doesn’t need to check an option box or sign and date the notice when you issue the ABN as a voluntary notice.
Option 1
The patient wants to get the items or services listed and accepts financial responsibility if we don’t pay. They agree to pay now, if required. Notifiers must submit a claim to Medicare that results in a payment decision the patient can appeal. If they need a Medicare claim denial for secondary insurance to cover the service, advise them to select Option 1.
Special guidance for non-participating suppliers and providers (those who don’t accept Medicare assignment) ONLY:
Strike the last Option Box 1 sentence as shown here:
□ OPTION 1. I want the D. ___________ listed above. You may ask for payment now, but I also want Medicare billed for an official decision on payment, sent to me, on a Medicare Summary Notice (MSN). I understand if Medicare doesn’t pay, I am responsible for payment, but I can appeal to Medicare by following the MSN directions. If Medicare does pay, you will refund any payments I made to you, less co-pays or deductibles.
Notifiers include this single line strike on ABNs printed specifically when you provide unassigned items and services. You can also hand-pen the line on an already-printed ABN. Don’t entirely conceal or delete the sentence. We don’t require you or patients to initial beside the sentence or date the annotations when you make the changes.
When you strike this sentence, include this CMS-approved unassigned claim statement in the (H) Additional Information section:
“This supplier doesn’t accept Medicare payment for the item(s) listed in the table above. If I checked Option 1 above, I am responsible for directly paying the supplier’s charge for the item(s). If Medicare does pay, Medicare will pay me the Medicare-approved amount for the item(s), and this payment may be less than the supplier’s charge.”
You can include this statement on ABNs printed for unassigned items and services or hand-write it in a legible 10 point or larger font.
Fourth ABN D. Field
Use the same wording used in the first (D) field.
Fifth ABN D. Field
Use the same wording used in the first (D) field.
Sixth ABN D. Field
Use the same wording used in the first (D) field.
Option 2
The patient wants to get the item or service listed and accepts financial responsibility. They agree to pay now, if required. When the patient chooses this option, you don’t file a claim, and they don’t have appeal rights.
You won’t violate mandatory claims submission rules under Section 1848 of the Social Security Act when you don’t submit a claim at the patient’s written request.
Option 3
The patient doesn’t want the care in question, and you can’t charge them for items or services listed. You don’t file a claim, and the patient doesn’t have an appeal right.
H. Additional Information
Notifiers can use this space to clarify what they believe is useful to patients. You may use this space to include:
- A statement advising the patient to notify their provider about certain tests that were ordered but not received
- Information on other patient insurance coverage, like a Medigap policy
- An additional dated witness signature
- Other necessary annotations
We assume notifiers make annotations on the same date that appears in field (J), accompanying their signature. If you make annotations on different dates, make those dates part of the annotations.
Signing below means that you received and understand this notice. You ask to receive a copy.
I. Signature
The patient (or their representative) must sign the notice to indicate they got it and understand its contents. If a representative signs for the patient, they should write “representative” in parentheses after their signature. The representative’s name should be clearly legible or noted in print.
J. Date
The patient (or their representative) must write the date they signed the ABN. If the patient has physical difficulty writing and requests assistance completing this field, you may write the date.
Resources
Disclaimers
View the Medicare Learning Network® Content Disclaimer and Department of Health & Human Services Disclosure.
The Medicare Learning Network®, MLN Connects®, and MLN Matters® are registered trademarks of the U.S. Department of Health & Human Services (HHS).