We added guidance for skilled nursing facilities (SNFs) on the appropriate methods for providers to determine their allowable related-party costs.
Substantive content changes are in dark red.
Skilled Nursing Facility Stays
Medicare Part A covers Medicare-certified skilled nursing facility (SNF) skilled care. Skilled care is nursing or other rehabilitative services, provided according to physician orders, that:
Require skills of qualified technical or professional health personnel, like:
Registered nurses
Licensed practical or vocational nurses
Physical therapists
Occupational therapists
Speech-language pathologists or audiologists
Skilled nursing or skilled rehabilitation personnel, or others under their general supervision, provide:
Supervision requiring initial direction and periodic inspection of the actual activity
Services that an assistant performs when a supervisor isn’t always physically present or at the location
We consider a service skilled if, because of its complexity, you can only perform it safely and effectively by, or under the supervision of, skilled nursing or skilled rehabilitation personnel.
Fee-for-Service (FFS) Medicare (also known as Original Medicare) enrollees must meet these conditions to qualify for Part A-covered SNF services:
Patient was a hospital inpatient for a medically necessary stay of at least 3 consecutive calendar days
Time spent in observation or in an emergency department doesn’t count toward a medically necessary 3-day qualifying inpatient hospital stay
A Medicare Advantage (MA) plan, 1876 Cost plan, Program of All-inclusive Care for the Elderly (PACE) plan, or SNFs that have a relationship with Shared Savings Program Accountable Care Organizations (ACOs) may waive the 3-day stay for their enrollees
Patient transfers to a Medicare-certified SNF within 30 days after hospital discharge, unless both are true:
Patient’s condition is medically inappropriate for starting active treatment in a SNF immediately after discharge
It’s medically predictable at the patient’s hospital discharge that they’ll need covered SNF care within a predetermined period, and they meet that prediction
Patient needs daily skilled nursing or rehabilitation services
Daily skilled services happen only in a SNF on an inpatient basis if:
They aren’t available on an outpatient basis in the patient’s location
Compared to an inpatient setting, transportation to a facility is:
An excessive physical hardship
Less economical
Less efficient or effective
Services are reasonable and necessary for diagnosing or treating a patient’s qualifying condition and of reasonable duration and quantity
We measure SNF coverage in benefit periods, sometimes called “spells of illness.” It starts the day a hospital or SNF admits a patient as an inpatient.
A benefit period ends after a patient isn’t an inpatient of a hospital or SNF for 60 consecutive days. Once a benefit period ends, a new benefit period starts when a hospital or SNF admits a patient. New benefit periods don’t start with a change in diagnosis, condition, or CY.
SNFs need to understand benefit periods because sometimes they must submit claims even when they don’t expect payment. This ensures proper tracking in the Common Working File (CWF), which Medicare Administrative Contractors (MACs) use to verify SNF benefit periods and patient information.
For each benefit period, Part A covers up to 20 full days of care. After that, Part A covers up to an additional 80 days, with the patient paying coinsurance for each day.
After 100 days, the SNF coverage available during that benefit period exhausts, and the patient pays for all care, except certain Medicare Part B services.
Medicare drug plan (Part D) coverage may be available to a Part D patient who’s exhausted their Part A inpatient stay benefit but remains in that inpatient setting, if the drug would otherwise be covered under Part D. Medicare Prescription Drug Benefit Manual, Chapter 6, section 20.2.1 has more information.
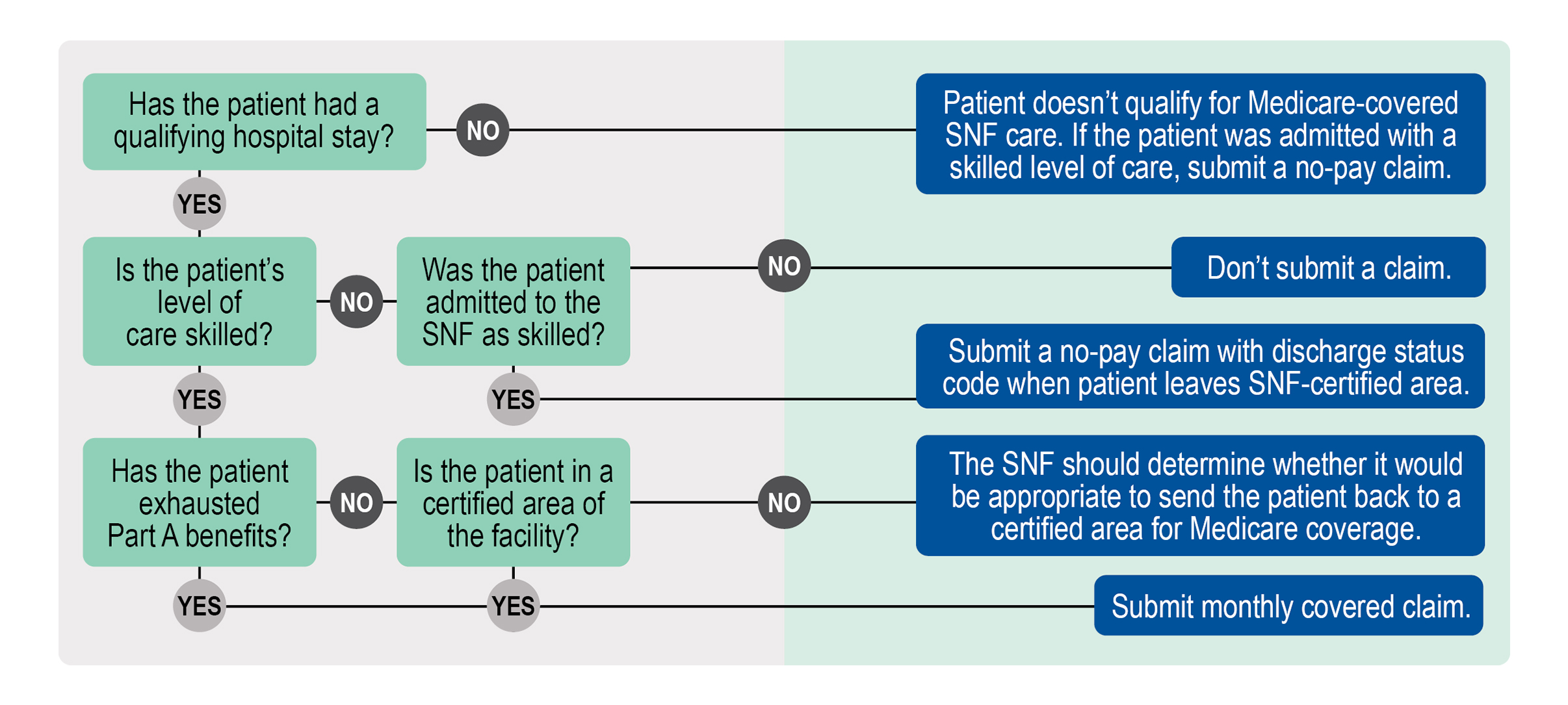
This figure describes the relationships between coverage, skilled care, the benefit period, and type of claim, if any, to submit to us:
SNF Coverage & Billing Summary
Providers should communicate with patients about:
Whether SNF care is right for them — Medicare skilled care can manage the patient’s current condition by preventing or slowing further deterioration.
SNF coverage requirements — Determine if the patient meets SNF coverage requirements before ordering SNF care. Part A won’t cover the SNF care if it isn’t medically reasonable and necessary or is considered custodial care.
Issue the Advance Beneficiary Notice of Non-coverage (CMS-R-131) (ABN) for Part B items or services that we may deny if they aren’t medically reasonable and necessary to transfer potential financial liability to the patient
SNF Part B Billing
Bill repetitive services to Part B monthly or when treatment stops. Bill one-time services to Part B when you complete the service. Medicare Claims Processing Manual, Chapter 7 has more information.
MA plans typically waive the 3-day hospitalization requirement. MA plans must cover the same number of SNF days FFS Medicare covers, but they may cover more.
Note: For MA plan patients, check with the MA plan for information on eligibility, coverage, and payment. Each plan can have different patient out-of-pocket costs and specific rules for getting and billing for services.
Follow the plan’s payment terms and conditions:
MA plans may offer different benefit periods.
Each MA plan’s Evidence of Coverage describes its benefits, including SNF coverage.
Most MA plans offer SNF coverage through network providers paid according to their contracts. Non-network SNFs should confirm MA coverage with the patient’s MA plan.
MA plans that cover SNF services provided by non-network SNFs pay the FFS Medicare payment rate, consistent with MA regulations at 42 CFR 422.214.
Payment
We pay for SNF services per diem under a prospective payment system (PPS). The SNF PPS per diem payment covers all Part A SNF services (routine, ancillary, and capital-related costs), except approved educational activities and services excluded from SNF Consolidated Billing (CB) costs under section 1888(e)(4)(E) of the Social Security Act.
We base Part A payment primarily on the patient’s assigned case-mix classification. We use the ICD-10-CM codes on the Minimum Data Set (MDS) in Item I0020B and map these codes to a Patient Driven Payment Model (PDPM) clinical category.
PDPM helps decide payment by classifying SNF patients in covered Part A stays. It affects PPS payments by:
Improving payment accuracy by focusing on patient characteristics rather than number of services provided
Reducing administrative provider burdens
Improving SNF payments to underserved patients without increasing total payments
We bundle payment for most patient services in a covered Part A SNF stay, including most services provided by entities other than the SNF. SNFs must bill these bundled services to their MAC in a CB. If you or your entity delivered services subject to CB and aren’t the SNF, don’t bill Medicare; bill the SNF.
When we disqualify a patient’s SNF Part A coverage, CB rules don’t apply. The following situations are reasons for disqualification:
Part A benefits exhaust
No qualifying 3-day hospital stay
Level-of-care requirement not met
There’s no comprehensive institutional coverage like under Part A for a non-covered Part B stay. However, the patient may qualify for Part B medical coverage and other individual health services.
We may pay for:
Outpatient hospital services to patients who aren’t SNF inpatients:
Diagnostic tests like diagnostic X-rays or lab tests
Physical therapy, occupational therapy, or speech-language pathology services
Physician and surgeon services
Services excluded from SNF PPS and SNF CB
Certain medical and other health services to patients residing in a SNF whose Part A benefits exhausted or who aren’t otherwise entitled to Part A payment
When a patient’s benefits exhaust, follow the guidance in Table 3 to make sure the claims processing system accurately tracks the benefit period.
Medicare Claims Processing Manual, Chapter 25 has CMS-1450 general billing information. SNFs must also populate the Table 1 elements for Part A claims. Complete these fields for all claims.
Table 1. SNF Billing Requirements
UB-04 Field
Report
Form Locator (FL) 04
Type of Bill (TOB)
21X for SNF inpatient services.
18X for hospital swing bed services.
FL 06
Statement Covers Period (From and Through dates)
From date must be the admission date or, for a continuing stay bill, the day after the Through date on the previous bill.
Through date is the last day of the billing period.
70 with the dates of the 3-consecutive-day qualifying stay.
FL 42
Revenue Code
0022 to show you’re submitting the claim under the SNF PPS. You can use this revenue code as often as necessary to show different HIPPS rate codes and assessment periods.
FL 44
HCPCS/Rate/HIPPS Rate Code
HIPPS rate code (SNF billing practices related to HIPPS codes stay the same under PDPM).
Must be in the same order the patient got that level of care. Certain HIPPS rate codes need more rehabilitation therapy ancillary revenue codes. If you don’t include the corresponding codes, your MAC returns the claims for re-submission.
FL 46
Units of Service
Number of covered days for each HIPPS rate code.
FL 47
Total Charges – Not Applicable for Electronic Billers
We won’t pay under the SNF PPS unless you bill a covered day.
We only allow ancillary charges for covered days and those included in the PPS rate.
Bill in order. MACs return a continuing stay bill if they haven’t processed the previous bill. If you submitted the previous bill, hold the returned continuing stay bill until you get the remittance advice for the previous bill.
Don’t count the day of discharge or death, or a day when a patient starts a leave of absence (LOA), as a utilization day.
If a facility discharges a patient who returns before the following midnight, we don’t count it as a discharge.
The HIPPS rate code on the claim must match the assessment that’s submitted and accepted by the CMS national database, the iQIES system.
For help with other billing situations, find your MAC’s website.
It’s important for SNFs to know when to bill a patient’s prescription drugs to Part A, instead of their Part D drug plan, to prevent improper payments:
Drugs prescribed for a Part D-enrolled patient aren’t covered by Part D if Part A or B can pay for them
Part A covers drugs and biologicals ordinarily provided by SNFs for the patient’s care and treatment
Part A covers a limited supply of drugs to use outside a SNF if it’s medically necessary to help a patient leave the facility and is required until they can get a continuing supply
Place of service (POS) codes identify where a patient gets a service. Enter the correct 2-digit code on Medicare claims to ensure proper payment for physician services provided to patients in inpatient facilities like SNFs and hospitals. POS codes frequently associated with SNF services include:
Inpatient hospital: 21
SNF (with Part A coverage): 31
Nursing facility (or SNF patient with no Part A coverage): 32
A recent Office of Inspector General report revealed that physicians sometimes enter POS code 32, indicating they provided patient services in a nursing facility or during a non-covered SNF stay, when, in fact, the patient was covered under Part A. Use POS code 31 for services you provide during a Part A stay in a SNF.
Additionally, if a patient is seen in a physician’s office but is also:
Certain situations require different approaches from the billing practices we discussed above. In these cases, submit a no-pay claim even though you don’t expect payment. The information in Tables 2–7 helps you decide how to bill various Part A situations. Remember to supply adequate claims-supporting documentation for reported services.
Readmission happens when the SNF discharges and readmits a patient for skilled care within 30 days after the discharge day. The patient can resume using available SNF benefit days without another qualifying hospital stay. The same is true if the patient stays in the SNF for custodial care after a covered stay and then develops a new skilled care need within 30 consecutive days after the first day of non-coverage.
Table 2. Readmitted Within 30 Days After Discharge Situations
If…
Then…
You sent a discharge claim before readmission
Submit another bill and report:
Current stay admission date
Condition code 57
Occurrence span code 70 with the qualifying hospital stay dates of at least 3 days
You readmit a patient before you send a discharge claim
Submit an interim bill and report:
Current stay admission date
Condition code 57
Occurrence span code 70 with the qualifying hospital stay dates of at least 3 days
Occurrence span code 74 showing the LOA From and Through dates and the number of non-covered days
When benefits exhaust, continue submitting monthly bills if the patient stays in a Medicare-certified area of the facility. Benefits can exhaust:
Fully — Patient had no benefit days available between the From and Through dates on the claim
Partially — Patient had benefit days available between the From and Through dates on the claim
Table 3. Benefits Exhaust Situations
If…
Then…
Patient moves to a non-Medicare-certified area of the institution
Discharge them using the correct discharge status code.
If appropriate, the claims processing system applies an A3 occurrence code with the last day the patient had benefits.
Report:
Covered TOB except for 210 or 180
HIPPS ZZZZZ
Occurrence span code 70 with qualifying hospital stay dates
Covered days and charges as if the patient had days available
Value code 09 (first year coinsurance amount) = $1
Patient status code
Don’t submit Part B services with TOB 22X until the benefits exhaust claim processes. Submit Part B services delivered after skilled care ended, including therapy, on a TOB 22X.
Patient drops to a non-skilled level of care while benefits exhaust and stays in a Medicare-certified area of the institution
Report:
TOB 212 or 213 for SNF and 182 or 183 for swing bed; don’t report TOBs 210 or 180
Occurrence span code 70 with qualifying hospital stay dates
Occurrence code 22 with date covered SNF care ended
Covered days and charges as if the patient had days available
Value code 09 (first year coinsurance amount) = $1
Patient status code 30 (still patient)
Submit Part B services delivered after skilled care ended, including therapy, on a TOB 22X.
Patient drops to a non-skilled level of care while benefits exhaust and moves to a non-Medicare-certified area of the institution or otherwise discharges
Report:
TOB 211 or 214 for SNF and 181 or 184 for swing bed; don’t report TOBs 210 or 180
Covered days and charges as if the patient had days available
Value code 09 (first year coinsurance amount) = $1
Patient status code, use appropriate code other than patient status code 30
Submit Part B services delivered after skilled care ended, including therapy, on a TOB 23X.
For no-payment billing, the patient drops to a non-skilled level of care and stays in a Medicare-certified area of the institution.
Table 4. No-Payment Billing Situations
If…
Then…
You need a denial notice so another insurer will pay
Send the initial no-payment claim with the From date as the date active SNF care ended. Then, continue to send claims as often as monthly.
Report:
TOB 210 for SNF or 180 for swing bed
All days and charges as non-covered, starting the day following the day SNF care ended
Condition code 21
Patient status code
HIPPS ZZZZZ
Submit Part B services delivered after skilled care ended, including therapy, on a TOB 22X.
You don’t need a denial notice
Send 1 final discharge claim, which may span both the SNF and Medicare FY end dates.
Report:
TOB 210 for SNF or 180 for swing bed
From date as the day Part A-covered SNF care ended
Through date as the discharge date
All days and charges as non-covered, starting the day following the day SNF care ended
Condition code 21
Patient status code (other than 30)
HIPPS ZZZZZ
Submit Part B services delivered after skilled care ended, including therapy, on a TOB 22X.
Provider-initiated discharges for coverage reasons related to SNF and inpatient swing bed claims need an expedited determination notice. A patient or a representative can appeal provider service terminations to a Beneficiary Family Centered Care-Quality Improvement Organization (BFCC-QIO) through the expedited review process.
BFCC-QIOs must inform the patient of:
Their right to an expedited reconsideration by the Qualified Independent Contractor (QIC)
How to ask for an expedited reconsideration
Report the outcomes of expedited determinations on the claim.
Table 5. Expedited Review Results Situations
If…
Then…
BFCC-QIO or QIC upholds the discharge decision
Report:
Discharge for billing period before the determination
Condition code C4
If the patient is liable for care days, report:
Occurrence span code 76 with the number of days the patient is liable
Zero charges for the patient-liable days
Modifier TS for any HCPCS codes for those days
BFCC-QIO or QIC authorizes continued coverage with no specific end date
Report:
Continuing claim for the current billing or certification period
Condition code C7
BFCC-QIO or QIC authorizes continued coverage only for a limited period, and the time extends beyond the end of the normal billing or certification period
Report:
Continuing claim for the current billing or certification period
Condition code C3
Occurrence span code M0 with the starting date of BFCC-QIO- or QIC-approved coverage and the claim Through date
BFCC-QIO or QIC authorizes continued coverage only for a limited period, and the time doesn’t extend beyond the end of the normal billing or certification period
Report:
Discharge claim
Condition code C3
Occurrence span code M0 with the starting and end dates of BFCC-QIO- or QIC-approved coverage
Provider is liable due to failure to give information promptly to the BFCC-QIO or QIC or deliver valid notice to the patient
Report services as non-covered with modifier GZ.
The patient doesn’t meet Medicare SNF coverage requirements.
Table 6. Non-Covered Days Situations
If…
Then…
Patient is liable
Report occurrence span code 76.
Submit the claim as covered if care is skilled.
SNF is liable
Report occurrence span code 77.
Submit the claim as covered if care is skilled.
Table 7. Other SNF Billing Situations
Situation
If…
Then…
No qualifying hospital stay
Facility admits a patient who needs skilled care but doesn’t have a qualifying hospital stay. This includes patients initially admitted as needing skilled care, following a qualifying hospital stay, who then dropped to a non-skilled level of care for more than 30 days. This ended their connection to the original qualifying hospital stay, and the patient’s care became skilled again without a new qualifying hospital stay.
Bill normally, but don’t report occurrence span code 70.
Same day transfer
SNF admits a patient who’s expected to stay overnight but transfers before the following midnight to a Medicare-participating facility.
Report:
Same admission From and Through dates
Zero covered days
Condition code 40
Leave of absence (LOA)
Patient leaves the SNF but isn’t admitted as an inpatient to any other facility.
Report:
Revenue code 018X
Number of LOA days as units
Zero charges
Occurrence span code 74 showing From and Through dates for the LOA and the number of non-covered days
Forced discharge
Patient leaves the SNF and is admitted as an inpatient to another facility.
Bill as a discharge. If the SNF readmits the patient within 30 days, follow the instructions in Table 2.
Non-skilled discharge
Patient drops to a non-skilled level of care and moves to a non-Medicare-certified area of the institution.
Discharge the patient on a final discharge claim. Submit services provided after discharge on TOB 23X.
Demand billing
SNF believes covered skilled care is no longer medically necessary, and the patient disagrees.
Report:
Condition code 20
Occurrence code 22 with the date SNF care ended or occurrence code 21 with the date you got the utilization review notice
MA plan information-only billing
Patient is an MA plan enrollee.
Submit information-only claims to Medicare so the CWF can track the benefit period.
Report:
Appropriate HIPPS code based on assessment or HIPPS ZZZZZ if no assessment happened
Room and board charges
Condition code 04
Disenroll from MA plan and enroll in FFS Medicare while SNF inpatient
Patient meets the level of care criteria through the effective disenrollment date.
We waive the qualifying hospital stay requirement and the patient is eligible for the number of days left out of the 100-day benefit period for that stay minus the days FFS Medicare would’ve covered while the patient was enrolled in an MA plan.
Report condition code 58.
Disenroll from MA plan after SNF discharge and enroll in FFS Medicare
Facility readmits a patient under the 30-day rule.
Patient must meet all FFS Medicare requirements, including qualifying 3-day hospital stay. Providers may charge patients for SNF coinsurance.
Report condition code 58.
Disenroll from MA plan
Patient disenrolls from MA plan before SNF admission.
Patient must meet all FFS Medicare requirements, including qualifying 3-day hospital stay.
Report condition code 58.
Interrupted stay
Patient is discharged from a Part A-covered stay and then resumes SNF care in the same SNF for a Part A-covered stay during a 3-day period, starting with the calendar day of Part A discharge and including the 2 calendar days immediately following (known as an interruption window).
We require an Omnibus Budget Reconciliation Act (OBRA) Discharge Assessment, as well as an entry tracking record on re-entry, but not a 5-day MDS assessment.
Medicare regulations and Provider Reimbursement Manual provisions require all providers and suppliers to submit Medicare cost reports. They must report related party costs—the actual cost incurred by the related organization, not the amount charged to the provider. We pay the lower of the supplier’s costs or the market price. Related party costs must not exceed the price of comparable services, facilities, or supplies available elsewhere. In a 2024 report, OIG found that SNFs didn’t report or had incorrect related parties’ costs on their Medicare cost reports despite Medicare’s requirements.
Report Accurate Related Party Costs
Report accurate related costs to prevent profit payments to the provider. The Medicare cost report data directly impacts Medicare payment rates, policy decisions, and the financial stability of the health care system. Accurate and complete reporting of all data on the Medicare cost reports ensures that we’re paying the appropriate amount to the correct provider for the proper service at the right time.
Maintain Documentation
Maintain accurate documentation of your related organization’s actual costs. This documentation must include:
Detailed identification of the organization’s total costs
Allocation basis for your direct and indirect costs to the provider
If an entity wishes to utilize any AHA materials, please contact the AHA at ub04@aha.org or 312-422-3366. Making copies or utilizing the content of the UB-04 Manual, including the codes and/or descriptions, for internal purposes, resale and/or to be used in any product or publication; creating any modified or derivative work of the UB-04 Manual and/or codes and descriptions; and/or making any commercial use of UB-04 Manual or any portion thereof, including the codes and/or descriptions, is only authorized with an express license from the American Hospital Association. The American Hospital Association (the “AHA”) has not reviewed, and is not responsible for, the completeness or accuracy of any information contained in this material, nor was the AHA or any of its affiliates, involved in the preparation of this material, or the analysis of information provided in the material. The views and/or positions presented in the material do not necessarily represent the views of the AHA. CMS and its products and services are not endorsed by the AHA or any of its affiliates.