June 15, 2026
Table of Contents
- Proposed Decision
- Proposed Decision
- Coverage Criteria
- Patient Criteria
- Physician and Heart Team Criteria
- Hospital Criteria
- CED Study Criteria
- Other Uses of TAVR
- Clinical Evidence Review
- Background
- Food and Drug Administration Status
- Review of the Evidence: Methods
- Evidence Questions
- Related Work
- Clinical Literature Search and Selection
- Quality Assessment
- Review of Evidence from Primary Studies
- Study Characteristics
- Key Findings
- Quality of Evidence from Primary Studies
- Applicability to the Medicare Population
- Supplemental Evidence and Guidance
- Evidence from Meta-analyses
- Evidence-based Guidelines / Professional Society Recommendations / Consensus Statements / Other Expert Opinion
- Appropriate Use Criteria
- Evidence Summary
- Public Comment
- CMS Coverage Analysis
- CMS Coverage Authority
- CMS Analysis of Coverage of TAVR for Aortic Stenosis
- Rationale for Proposed Coverage Criteria
- Evidence Questions - Answered
- Benefit Category
- Termination of CED
- Shared-Decision Making
- Quality Measures
- History of Medicare Coverage
- Previous National Coverage Analysis
- Current National Coverage Request
- Timeline of NCA Milestones
- Appendices
- Appendix A: Proposed Medicare National Coverage Determinations Manual Language
Appendix B: Referenced Materials and Supplemental Information
Bibliography
Abbreviations used throughout the Proposed Decision Memorandum for Transcatheter Aortic Valve Replacement (TAVR)
ACC – American College of Cardiology
AHA – American Heart Association
AHRQ – Agency for Healthcare Research and Quality
AS – Aortic Stenosis
AV – Aortic Valve
AVR – Aortic Valve Replacement
AATS – American Association for Thoracic Surgery
BEV – Balloon-Expandable Valve
CABG – Coronary Artery Bypass Grafting
CAV – Commercially Available Valves
CDC – Centers for Disease Control and Prevention
CI – Confidence Interval
CMS – Centers for Medicare & Medicaid Services
COPD – Chronic Obstructive Pulmonary Disease
COVID – Coronavirus Disease
CS – Clinical Surveillance
CV – Cardiovascular
DEDICATE-DZHK6 – Decisive Role of Transcatheter Aortic Valve Implantation Compared With Surgical Valve Replacement in Low-to-Intermediate-Risk Patients
EACTS – European Association for Cardio-Thoracic Surgery
eGFR – Estimated Glomerular Filtration Rate
ESC – European Society of Cardiology
ESRD – End-Stage Renal Disease
EuroSCORE – European System for Cardiac Operative Risk Evaluation
FDA – U.S. Food and Drug Administration
FU – Follow-up
GRADE – Grading of Recommendations Assessment, Development and Evaluation
HF – Heart Failure
HR – Hazard Ratio
ICD – Implantable Cardioverter Defibrillator
ITT – Intention-to-treat
KCCQ – Kansas City Cardiomyopathy Questionnaire
KM – Kaplan–Meier
LV – Left Ventricle
LRT – Low Risk TAVR
MCID – Minimal clinically important differences
MEDCAC – Medicare Evidence Development & Coverage Advisory Committee
MEV – Mechanically-Expandable Valve
MI – Myocardial Infarction
N/A – Not Applicable
NOTION – Nordic Aortic Valve Intervention
NCA – National Coverage Analysis
NS – Not Statistically Significant
NYHA – New York Heart Association
OR – Odds Ratio
PARTNER – Placement of Aortic Transcatheter Valves
PICOTS – Population, Intervention, Comparator, Outcomes, Timing, Setting
RCT – Randomized Controlled Trial
RHEIA trial - Randomized researcH in womEn all comers wIth Aortic stenosis
RR – Relative Risk
SAVR – Surgical Aortic Valve Replacement
SCAI – Society for Cardiovascular Angiography and Interventions
SD – Standard Deviation
SEV – Self-Expanding Valve
SHD – Structural Heart Disease
SLR – Systematic Literature Review
SMART – Small Annuli Randomized to Evolut or SAPIEN Trial
SOLVE TAVI - CompariSon of secOnd-generation seLf-expandable vs. balloon-expandable Valves and gEneral vs. local anaesthesia in Transcatheter Aortic Valve Implantation
STS PROM – Society of Thoracic Surgeons Predicted Risk of Mortality
SURTAVI – Surgical Replacement and Transcatheter Aortic Valve Implantation
TAVR – Transcatheter Aortic Valve Replacement
TVT – Transcatheter Valve Therapy
USPSTF – U.S. Preventive Services Task Force
VARC – Valve Academic Research Consortium
VHD – Valvular Heart Disease
Throughout this NCD, we use “symptomatic severe aortic stenosis” interchangeably with, but preferentially to, the term “severe symptomatic aortic stenosis” (seen commonly in the medical literature), with the intent of clarifying that it is the stenosis itself that is severe, not necessarily the symptoms.
I. Proposed Decision
The Centers for Medicare & Medicaid Services (CMS) proposes to: 1) cover Transcatheter Aortic Valve Replacement (TAVR) for symptomatic severe aortic valve stenosis (or aortic stenosis (AS)) without the coverage with evidence development (CED) requirement; 2) expand coverage of TAVR to asymptomatic severe AS with CED; 3) revise coverage criteria related to pre-procedural patient assessment, intraoperative requirements, and operator and hospital procedural volume requirements.
We propose that TAVR for severe AS is covered when furnished with a complete aortic valve and implantation system that has received Food and Drug Administration (FDA) premarket approval (PMA) for that system’s FDA-approved indication, and the following conditions are met.
TAVR is covered for the treatment of Medicare beneficiaries with:
- Symptomatic severe AS under § 1862(a)(1)(A) of the Social Security Act (the Act).
- Asymptomatic severe AS under CED, § 1862(a)(1)(E) of the Act.
Provisions in B2 and B3 below apply to all TAVR procedures furnished under the NCD; provision B4 applies only to TAVR procedures furnished under CED.
2. Physician and Heart Team Criteria
Heart Team: The patient (preoperatively and postoperatively) is under the care of a heart team: a cohesive, multi-disciplinary team of medical professionals with a specialized focus in cardiac care. The heart team concept embodies collaboration and dedication across medical specialties to offer optimal patient-centered care. The heart team:
- Must include at least one cardiac surgeon and one interventional cardiologist experienced in the care and treatment of AS and each with clinical privileges at the hospital where the TAVR will be furnished; and
- May include other physicians, advanced practice clinicians, and nurses, as well as research personnel and administrators.
Patient Evaluation: Suitability for surgical aortic valve replacement (SAVR), TAVR, close surveillance, and palliative care must be evaluated based on individual clinical, anatomical, and procedural characteristics, lifetime management considerations, and estimated patient life expectancy. These evaluations must be documented and made available to other heart team members, the patient, and other clinicians involved in the patient’s care as appropriate, prior to the day of the procedure. Evaluations must include:
- An initial evaluation by the heart team, which could be asynchronous using medical records to identify patient suitability for TAVR or other treatments; and
- An independent, in person evaluation by a heart team TAVR operator. This cannot be satisfied through a virtual encounter.
TAVR Operator: A TAVR operator must be an interventional cardiologist or cardiac surgeon member of the heart team and:
- Perform ≥ 20 total transcatheter cardiac valve (including aortic, mitral, tricuspid, or pulmonic valve) procedures, ≥ 15 of which must be TAVR, every year; or
- Perform ≥ 40 such procedures, ≥ 30 of which must be TAVR, every two years.
Joint participation of two TAVR operators in a TAVR procedure is not required but may occur if determined appropriate by the heart team. If jointly performed, both must be TAVR operators from the heart team.
TAVR procedures must be furnished in a hospital with the appropriate infrastructure that includes but is not limited to:
- On-site structural heart interventional cardiology and cardiac surgery programs.
- A post-procedure intensive care unit with personnel experienced in managing patients who have undergone open-heart valve procedures.
- A continuous quality improvement process that assesses procedural outcomes and makes necessary programmatic adjustments to assure patient safety.
TAVR items and services are furnished for the treatment of asymptomatic severe AS with a complete aortic valve and implantation system that has received FDA PMA for that system’s FDA-approved indication in the context of a CMS-approved CED study.
CED studies must meet requirements of sections B2 (Physician and Heart Team Criteria) and B3 (Hospital Criteria), have an active, contemporaneous comparator and address at least one of the following questions:
- Does TAVR, SAVR, or close surveillance until symptom onset better improve health outcomes? This is particularly relevant for patients with lower surgical risk, longer life expectancy, preserved left ventricular ejection fraction, and bicuspid aortic valves.
- What are the long-term valve re-intervention rates of TAVR vs SAVR and does having re-interventions impact health outcomes?
- Can longer term, risk-standardized, patient-centered health outcomes replace volume criteria for TAVR operators?
Any future reconsideration of this NCD would consider answers to all of these CED questions, and the totality of extant evidence in the published, peer-reviewed medical literature, to assess whether use of TAVR for AS improves health outcomes for Medicare beneficiaries.
CMS-approved CED studies must adhere to the following scientific standards (criteria 1-17 below) that have been identified by the Agency for Healthcare Research and Quality (AHRQ) as set forth in Section VI of CMS’ Coverage with Evidence Development Guidance Document, published August 7, 2024 (the “CED Guidance Document”).
- Sponsor/Investigator: The study is conducted by sponsors/investigators with the resources and skills to complete it successfully.
- Milestones: A written plan is in place that describes a detailed schedule for completion of key study milestones, including study initiation, enrollment progress, interim results reporting, and results reporting, to ensure timely completion of the CED process.
- Study Protocol: The CED study is registered with ClinicalTrials.gov and a complete final protocol, including the statistical analysis plan, is delivered to CMS prior to study initiation. The published protocol includes sufficient detail to allow a judgment of whether the study is fit-for-purpose and whether reasonable efforts will be taken to minimize the risk of bias. Any changes to approved study protocols should be explained and publicly reported.
- Study Context: The rationale for the study is supported by scientific evidence and study results are expected to fill the specified CMS-identified evidence deficiency and provide evidence sufficient to assess health outcomes.
- Study Design: The study design is selected to safely and efficiently generate valid evidence of health outcomes. The sponsors/investigators minimize the impact of confounding and biases on inferences through rigorous design and appropriate statistical techniques. If a contemporaneous comparison group is not included, this choice should be justified, and the sponsors/investigators discuss in detail how the design contributes useful information on issues such as durability or adverse event frequency that are not clearly answered in comparative studies.
- Study Population: The study population reflects the demographic and clinical diversity among the Medicare beneficiaries who are the intended population of the intervention, particularly when there is good clinical or scientific reason to expect that the results observed in premarket studies might not be observed in older adults or subpopulations identified by other clinical or demographic factors.
- Subgroup Analyses: The study protocol explicitly discusses beneficiary subpopulations affected by the item or service under investigation, particularly traditionally underrepresented groups in clinical studies, how the inclusion and exclusion requirements effect enrollment of these populations, and a plan for the retention and reporting of said populations in the trial. In the protocol, the sponsors/investigators describe plans for analyzing demographic subpopulations as well as clinically-relevant subgroups as identified in existing evidence. Description of plans for exploratory analyses, as relevant subgroups emerge, are also included.
- Care Setting: When feasible and appropriate for answering the CED question, data for the study should come from beneficiaries in their expected sites of care.
- Health Outcomes: The primary health outcome(s) for the study are those important to patients and their caregivers and that are clinically meaningful. A validated surrogate outcome that reliably predicts these outcomes may be appropriate for some questions. Generally, when study sponsors propose using surrogate endpoints to measure outcomes, they should cite validation studies published in peer-reviewed journals to provide a rationale for assuming these endpoints predict the health outcomes of interest. The cited validation studies should be longitudinal and demonstrate a statistical association between the surrogate endpoint and the health outcomes it is thought to predict.
- Objective Success Criteria: In consultation with CMS and AHRQ, sponsors/investigators establish an evidentiary threshold for the primary health outcome(s) so as to demonstrate clinically meaningful differences with sufficient precision.
- Data Quality: The data are generated or selected with attention to provenance, bias, completeness, accuracy, sufficiency of duration of observation to demonstrate durability of health outcomes, and sufficiency of sample size as required by the question.
- Construct Validity: Sponsors/investigators provide information about the validity of drawing warranted conclusions about the study population, primary exposure(s) (intervention, control), health outcome measures, and core covariates when using either primary data collected for the study about individuals or proxies of the variables of interest, or existing (secondary) data about individuals or proxies of the variables of interest.
- Sensitivity Analyses: Sponsors/investigators will demonstrate robustness of results by conducting pre-specified sensitivity testing using alternative variable or model specifications as appropriate.
- Reporting: Final results are provided to CMS and submitted for publication or reported in a publicly accessible manner within 12 months of the study’s primary completion date. Wherever possible, the study is submitted for peer review with the goal of publication using a reporting guideline appropriate for the study design and structured to enable replication. If peer-reviewed publication is not possible, results may also be published in an online publicly accessible registry dedicated to the dissemination of clinical trial information such as ClinicalTrials.gov, or in journals willing to publish in abbreviated format (e.g., for studies with incomplete results).
- Sharing: The sponsors/investigators commit to making study data publicly available by sharing data, methods, analytic code, and analytical output with CMS or with a CMS-approved third party. The study should comply with all applicable laws regarding subject privacy, including 45 CFR § 164.514 within the regulations promulgated under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and 42 CFR, Part 2: Confidentiality of Substance Use Disorder Patient Records.
- Governance: The protocol describes the information governance and data security provisions that have been established to satisfy Federal security regulations issued pursuant to HIPAA and codified at 45 CFR Parts 160 and 164 (Subparts A & C), United States Department of Health and Human Services (HHS) regulations at 42 CFR, Part 2: Confidentiality of Substance Use Disorder Patient and HHS regulations at 45 CFR Part 46, regarding informed consent for clinical study involving human subjects. In addition to the requirements under 42 CFR and 45 CFR, studies that are subject to FDA regulation must also comply with regulations at 21 CFR Parts 50 and 56 regarding the protection of human subjects and institutional review boards, respectively.
- Legal: The study is not designed to exclusively test toxicity or disease pathophysiology in healthy individuals, although it is acceptable for a study to test a reduction in toxicity of a product relative to standard of care or an appropriate comparator. For studies that involve researching the safety and effectiveness of new drugs and biological products aimed at treating life-threatening or severely-debilitating diseases, refer to additional requirements set forth in 21 CFR § 312.81(a).
Consistent with section 1142 of the Act, AHRQ supports clinical research studies that CMS determines meet all the criteria and standards identified above.
In addition to the national coverage described above, Medicare Administrative Contractors (MACs) may make reasonable and necessary determinations under section 1862(a)(1)(A) for any other beneficiary seeking coverage for TAVR for AS. This NCD does not apply to use of TAVR in emergency scenarios.
Nothing in this NCD precludes coverage of TAVR for AS through NCD 310.1 (Clinical Trial Policy) or through the Investigational Device Exemption (IDE) Policy.
Ongoing studies that were previously approved under CED for TAVR have been determined to meet requirements for, and are approved under, either section B4 of this NCD or the Investigational Device Exemption (IDE) regulations (42 CFR § 405 Subpart B). Ongoing studies, as specified on clinicaltrials.gov, will either continue to be posted to the CMS website of approved TAVR CED studies or will be moved to the CMS website of approved IDE studies upon finalization of this NCD.
See Appendix A for proposed Medicare National Coverage Determinations Manual language.
CMS is seeking comments on our proposed decision. We will respond to public comments in a final decision memorandum, as required by §1862(l)(3) of the Act.
II. Clinical Evidence Review
Aortic stenosis (AS) is a valvular heart disease in which the aortic valve narrows and does not open fully, restricting blood flow out of the heart. The left ventricle (one of four heart chambers) pumps oxygenated blood through the aortic valve to the aorta (the main artery) and then to the brain and rest of the body (https://www.mayoclinic.org/diseases-conditions/aortic-stenosis/symptoms-causes/syc-20353139).
AS is the most common valvular heart disease requiring intervention in the Medicare population. Over 12% of Medicare beneficiaries (age ≥65 years) have AS, with > 3% having severe AS (Martin 2024). Severity of stenosis increases with age. AS is usually caused by degenerative, age-related calcification, a congenital bicuspid aortic valve, or rheumatic fever. Symptoms typically occur in late-stage disease, when the stenosis is severe. The “classic” presentation is a triad of heart failure symptoms (dyspnea, or shortness of breath, and fatigue), syncope/ presyncope (fainting/dizziness), and angina (chest pain). However, this “classic triad” is less commonly seen in clinical practice today. Increasingly, patients with subtle or no symptoms have their AS diagnosed by an echocardiogram performed for other indications, or when a heart murmur is heard by stethoscope on physical exam.
AS is a progressive, fatal disease, with one large, U.S. multi-hospital, real-world database study reporting approximately 45% 4-year mortality for patients with untreated severe AS (Généreux 2023). The definitive treatment for AS is aortic valve replacement (AVR). Transcatheter AVR (TAVR) has emerged as a minimally invasive alternative to surgical AVR (SAVR) for treating AS. A bioprosthetic valve is inserted via a catheter, typically entered through an artery in the groin, into the opening of a native aortic valve or a failed surgical bioprosthetic aortic valve. Since the CMS national coverage determination (NCD) for TAVR in 2012, TAVR has become the predominant method for AVR for patients with symptomatic severe AS in the U.S. (Sherwood 2025).
Patients with asymptomatic severe AS have typically been managed with active surveillance, including periodic echocardiography, symptom assessment, and sometimes supervised exercise testing (Otto 2021). This is because the risk of sudden death in asymptomatic severe AS is low (≤1% per year), and there are competing risks associated with the procedure itself (Généreux 2016; Lancellotti 2018).
This proposed decision memorandum reconsiders the 2019 TAVR NCD, and was opened after a formal request by Edwards Lifesciences, manufacturer of the Sapien family of TAVR devices, following FDA expanded indications on April 30, 2025 to include asymptomatic as well as symptomatic patients with severe AS.
B. Food and Drug Administration Status
On November 2, 2011, the FDA approved the first TAVR device for marketing in the United States. The Edwards’ SAPIEN Transcatheter Heart Valve (THV) was approved "for transfemoral delivery in patients with severe symptomatic native aortic valve stenosis who have been determined by a cardiac surgeon to be inoperable for open AVR and in whom existing co- morbidities would not preclude the expected benefit from correction of the aortic stenosis" (https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P100041). Since this first approval, devices have been approved for:
- Lower surgical risk groups, including high and intermediate;
- Alternate access sites, such as transapical and transaortic;
- Valve-in-valve use for failed surgical bioprosthetic valves; and
- Asymptomatic AS.
Table 1 in Appendix B provides a timeline of TAVR device approvals to date.
C. Review of the Evidence: Methods
This NCD addresses TAVR for AS. It does not address TAVR for the treatment of other conditions like aortic regurgitation (AR).
This section describes how evidence from published clinical research regarding TAVR for AS was selected for consideration in this review.
A detailed account of the methodological principles used by CMS to assess the relevant literature on a therapeutic or diagnostic item or service for specific conditions can be found in the CMS National Coverage Analysis Evidence Review Guidance Document, published August 7, 2024, or any successor document.
The following questions guide our review and analysis of the selected evidence on the use of TAVR for AS:
Q1: Is the evidence sufficient to conclude that TAVR meaningfully improves health outcomes for Medicare beneficiaries with AS?
Q2: Do specific characteristics or comorbidities make patients more or less likely to benefit from TAVR?
Q3: Are specific treatment conditions necessary to achieve TAVR health outcomes similar to those demonstrated in the clinical studies reviewed in this analysis?
We used contractor support to conduct the literature searches and evidence review and supplemented that review with our own CMS coverage analysis.
i. Key Technology Assessments and Systematic Reviews
CMS did not request an external technology assessment (TA) on this topic.
ii. Medicare Evidence Development and Coverage Advisory Committee (MEDCAC)
A MEDCAC meeting was not convened on this topic.
3. Clinical Literature Search and Selection
Using contractor support, the evidence review began with a systematic search of the peer-reviewed literature in PubMed and Embase conducted on Nov 13, 2025, using the following primary search terms: (1) “Asymptomatic;” (2) “Aortic Valve Stenosis;”"[Mesh] (3) “aortic stenosis;” (4) “Transcatheter Aortic Valve Replacement,” [Mesh] or “Transcatheter aortic valve implantation.” The search was restricted to English-language articles published between 2018 and 2025. Primary studies were eligible for detailed analysis if they evaluated TAVR for AS, regardless of clinical or geographic setting, symptom status, or risk factors. They were also eligible for inclusion in this review if they included adults with AS and evaluated the safety or effectiveness of TAVR. Since several eligible randomized controlled trials (RCTs) were available, the analysis focused on major RCTs; registry-based observational studies were considered as supplemental data from real-world data sources, and single-arm or non-randomized trials were excluded. Major RCTs were pivotal trials published in high-impact, peer-reviewed journals with a prespecified statistical analysis plan and had a multicenter design with multinational or multiregional participation to reduce site-specific bias and enhance external validity. The inclusion criteria were broad to include a diverse patient population.
Inclusion:
- Comparison of TAVR with any active comparator, such as surgery or clinical surveillance
- Assessment of one of the following post-TAVR outcomes: adverse events, durability of the TAVR device, quality of life, stroke, mortality
Exclusion:
- Fewer than 100 patients in the intervention arm
- Patients followed for less than 30 days after TAVR
Due to the paucity of data on asymptomatic AS patients, one publication reporting 138 asymptomatic patients (76 TAVR; 62 SAVR) from the Evolut Low Risk study was included in the analysis (Merhi et al., 2022).
Meta-analyses of primary studies investigating TAVR for AS were also eligible for consideration. Because meta-analyses may overlap to some extent with our selected primary studies and may include studies of varying quality, our analysis and evidence quality assessment focused on the selected primary studies. We considered the meta-analytic findings as supplemental evidence.
Our review assessed the quality of individual studies according to the principles outlined in the United States Preventive Services Task Force Procedure Manual, Appendix VI. Criteria for Assessing Internal Validity of Individual Studies. The review used a modified version of the GRADE (Grading of Recommendations Assessment, Development and Evaluation) system to assess the body of evidence for each outcome or outcome category. The USPSTF tool allows evaluation of the design and conduct of a study with an emphasis on internal validity (minimization of bias). The GRADE system facilitates an assessment of the certainty of the overall evidence for specific outcomes, considering both the quality and findings of individual studies.
Our selection of primary studies for detailed analysis included 17 RCTs reported in 29 publications. Additionally, three comparative and four registry-based noncomparative observational studies were selected. Collectively, these selections involved approximately 10,686 patients from RCTs and 457,598 patients from the observational studies treated with TAVR. As shown in Table 2 in Appendix B, approximately half the studies were conducted exclusively or partially in the United States.
Demographic Characteristics
Across the included studies, the mean/median age of participants ranged from 70 to 85 years. The proportion of women participants ranged from 21 to 100 percent. Only four studies provided specific data on ethnicity; the patients in these studies were predominantly White.
AS Symptom and Risk Groups
Across all 24 included studies, patients were diagnosed with severe AS, defined by elevated transvalvular pressure gradients and reduced aortic valve areas. The surgical risk categories were defined using a combination of standardized scoring systems, specific mortality thresholds, and multidisciplinary clinical assessments. The Society of Thoracic Surgeons Predicted Risk of Mortality (STS-PROM) score, often referred to as the “STS score,” was the primary metric used to classify patients into low, intermediate, high, or extreme risk (scores ranging from 0% to 100%, with higher scores indicating greater risk of death within 30 days after the procedure).
RCTs
Among the 17 studies derived from the RCTs, the study populations comprised asymptomatic severe AS in two studies (Evolut Low Risk Trial [subgroup analyses], EARLY TAVR) and symptomatic severe AS in the remaining studies. One study specifically evaluated patients with symptomatic severe AS and a small aortic annulus (area ≤ 430 mm) (SMART trial). Among studies involving symptomatic AS populations, patients spanned a range of surgical risk profiles, including low risk (N = 4 studies; Evolut Low Risk, NOTION, NOTION-2, and PARTNER 3), low-to-intermediate risk (N = 1 study; DEDICATE-DZHK6), intermediate risk (N = 3; PARTNER 2 cohort A, PARTNER 2 SAPIEN 3, SURTAVI), intermediate-to-high risk (N = 1 study; SOLVE TAVI), high risk (N = 4 studies; Medtronic Core Valve US High-Risk Pivotal Trial, PORTICO IDE, Choice, and REPRISE III ), and studies enrolling patients across all risk categories (N = 3 studies; SMART, RHEIA, GALILEO).
Patient Characteristics in Asymptomatic Severe Aortic Stenosis Trials
- Low surgical risk (generally defined as an STS-PROM score <4%; the mean score was 1.7% and 1.8% in the Evolut Low Risk and EARLY TAVR trials, respectively).
- Preserved left ventricular ejection fraction (LVEF) (≥ 50% in both Evolut Low Risk and EARLY TAVR trials).
- A negative exercise treadmill stress test. This was the gold standard for identifying asymptomatic patients in the EARLY TAVR trial.
- NYHA Functional class I designation, indicating no symptoms during ordinary physical activity; this identified asymptomatic status in the Evolut Low Risk trial.
Patient Characteristics in Symptomatic Severe Aortic Stenosis Trials
Low risk trials
- STS score ≤4%. Defined as STS ≤3% in the Evolut Low Risk Trial and ≤4% in the PARTNER 3 and NOTION-2 trials.
- Mean STS scores ranged from 1.1% to 3.0% among symptomatic low-risk patients of the Evolut Low Risk, NOTION, NOTION-2, and PARTNER 3 trials.
- NYHA class II–III symptoms. These were the predominant NYHA classes at baseline in most trials (Evolut Low Risk, NOTION, and PARTNER-3). Some trials reported the presence of NYHA class III or IV symptoms in approximately 23.8% to 51.0% of patients at baseline.
Low to intermediate risk trials
- Low risk was defined as a STS score ≤2%, and intermediate risk as a score of 2% to 4% (DEDICATE-DZHK6). Mean STS scores ranged from 1.8% to 1.9% (DEDICATE-DZHK6).
- NYHA class III or higher (˜46%), indicating moderate functional limitation (DEDICATE-DZHK6).
Intermediate risk trials:
- STS score between 3% and 15% augmented by overall clinical status and comorbidities not captured by the STS risk calculation, including frailty and disability (SURTAVI).
- The mean STS score of the enrolled population ended up being approximately 4.5%, representing a truly intermediate-risk population with well-balanced frailty indices.
- STS score between 4% and 8% (PARTNER 2 cohort A) for patient eligibility.
- Actual STS scores of enrolled patients ranged from 4.4% to 5.8% (PARTNER 2 cohort A, PARTNER 2 SAPIEN 3, SURTAVI).
- NYHA class III or IV symptoms (74% to 77% of patients in PARTNER 2 and ~55% to 60% in SURTAVI).
Intermediate to high risk trials:
- Median STS scores between 4.7% to 4.9%, with interquartile ranges (IQRs) extending from 3.0% to approximately 9–10% (SOLVE TAVI).
- NYHA class III or IV symptoms (63% to 66% of patients; only 11.6% were class I) (SOLVE TAVI).
- Median logistic European System for Cardiac Operative Risk Evaluation (EuroSCORE) I was 14.8% to 14.9% (IQR 8.7%–23.8%) (SOLVE TAVI).
- High risk defined as EuroSCORE ≥20% and/or STS risk score ≥10%, or other high-risk criteria by heart team consensus (SOLVE TAVI).
High risk trials:
- Mean STS scores of 5.6% to 7.6% (Medtronic Core Valve US High-Risk Pivotal Trial, CHOICE, and REPRISE III).
- Defined as STS score of 8% or higher, or for whom two cardiac surgeons concurred that the predicted risk of operative mortality was 15% or higher at 30 days after surgery (PORTICO IDE).
- Medtronic Core Valve US High-Risk Pivotal Trial defined high risk as subjects with an expected perioperative mortality of 15% or more (based on an investigator-estimated mortality or an STS score >10).
- Trials such as PORTICO IDE and REPRISE III allowed the local heart team to override or supplement STS scores based on clinical judgment.
- Extreme risk was defined as a probability of death or serious morbidity exceeding 50% by 30 days after surgery (PORTICO IDE, REPRISE III).
- Baseline functional limitation with ~60% to 63% of patients classified as NYHA class III (REPRISE III, PORTICO IDE).
- Patients with lower STS scores could still be categorized as high or extreme risk due to other clinical features, such as a porcelain aorta, hostile chest (due to prior radiation or surgery), severe pulmonary hypertension, or significant frailty (REPRISE III).
Observational studies
Among the seven observational studies, one (STS/ACC TVT-health status) evaluated minimally symptomatic or asymptomatic patients with AS, one (OCEAN-TAVI) included a mixed population of symptomatic and asymptomatic patients with severe AS, and the remaining five studies focused exclusively on symptomatic patients with severe AS. These studies defined risk categories using a combination of standardized surgical risk scores, clinical symptom status, and multidisciplinary heart team consensus (STS/ACC TVT Registry, OCEAN-TAVI Registry, SWEDEHEART registry). Risk was also categorized by baseline health status using the Kansas City Cardiomyopathy Questionnaire Overall Summary (KCCQ OS), where a score < 75 indicates moderate to severe symptoms and a score of ≥75 indicates minimal or no symptoms (STS/ACC TVT Registry-health status). The median KCCQ-OS ranged from 43 to 85, reflecting wide variability in baseline health status (STS/ACC TVT-health status). Furthermore, the determination of risk frequently relied on heart team consensus, which evaluates patients based on clinical eligibility and serious surgical morbidity risks that scoring algorithms may not fully capture (OCEAN-TAVI, RESPOND).
Low surgical risk
- Defined by an STS-PROM score of 3% or less and the absence of other high-risk comorbidities, such as frailty, porcelain aorta, or advanced liver disease (STS/ACC TVT Registry-health status, LRT).
- In large real-world registries, patients categorized as low risk or with minimal symptoms had median STS scores ranging from 1.6% to 3.2% (STS/ACC TVT Registry-temporal change analysis and SWEDEHEART).
Intermediate surgical risk:
- Mean STS-PROM scores ranged from 4.4% to 6.0% (RESPOND Study).
High surgical risk:
- Defined as a patient being considered "unsuitable" for SAVR, with high-risk symptomatic cohorts achieving mean STS-PROM values of up to 11.2% (OCEAN-TAVI).
- The median EuroSCORE II ranged from 2.5% to 9.2% (OCEAN-TAVI).
Comparators
While the majority of included studies (N = 13) reported comparisons of TAVR with SAVR (including three from observational studies), six studies (all RCTs) reported head-to-head comparisons of different transcatheter heart valve systems. One RCT (EARLY TAVR) compared TAVR with clinical surveillance rather than surgery or a different valve type. Four observational studies (STS/ACC TVT-health status, STS/ACC TVT-temporal change analysis, OCEAN-TAVI, RESPOND study) focused on internal registry comparisons, such as changes in symptom status from baseline or temporal trends, rather than on a primary comparison with surgery or other valve systems. In one study, patients were not randomized to TAVR or SAVR; however, the analysis was adjusted for 25 important covariates in a propensity-matched analysis (PARTNER 2 SAPIEN 3). A variety of valves were used: self-expanding valves (SEV), balloon-expandable valves (BEV), and, to a lesser extent, mechanically expanded valves (MEV). In some studies, different patients received different valves. Overall, observational studies demonstrate greater valve heterogeneity than randomized trials, with substantial overlap between balloon-expandable and self-expanding platforms, and limited representation of mechanically expanded devices, confined to a single registry.
Setting and follow-up
Across studies, TAVR was delivered in hospital inpatient settings. Follow-up durations typically ranged from one to seven years. A small number of studies fell outside this range: three publications reported short-term outcomes with 30-day follow-up (Evolut Low Risk Trial; SOLVE TAVI; Low Risk TAVR), while one study reported extended long-term outcomes with follow-up of up to 10 years (NOTION).
Outcomes
A total of 81 outcomes were identified across the included studies: 17 primary and 37 secondary outcomes from RCTs, and an additional 27 outcomes from observational studies. The primary outcomes across RCTs and observational studies evaluated in this report include: composite of all-cause death, all stroke (disabling or non-disabling), or cardiovascular (CV) rehospitalization; composite of all-cause mortality or disabling stroke; composite of all-cause death or stroke; and composite safety outcome of death, stroke, stage 3 acute kidney injury/new dialysis, major, life-threatening, or disabling bleeding, and moderate or severe paravalvular regurgitation/leak. The secondary outcomes evaluated across RCTs and observational studies in this report include: all-cause mortality, CV mortality, stroke, disabling stroke, new permanent pacemaker implantation, myocardial infarction (MI), reintervention, patient-reported outcome using the KCCQ, bleeding, and rehospitalization.
Table 1 summarizes the characteristics and key findings of each study while Table 2 provides a summary of the evidence across studies.
a. Impact on Health Outcomes
Health outcomes are summarized first for RCTs and then for observational studies. Within each outcome, results are categorized by patient population (symptomatic, low-, intermediate-, and high-risk). Comparisons are reported in two stages: first, TAVR versus standard comparators such as SAVR or clinical surveillance (CS), and second, comparisons across different valve types where available. All percentages reported below are Kaplan–Meier estimates at the specific time point unless otherwise specified. Studies on asymptomatic patients are discussed separately in this section. The quality of evidence and study limitations are discussed in detail in Appendix B.
Randomized Controlled Trials – Symptomatic AS
All-cause mortality
Among the included studies reporting on all-cause mortality and survival, 11 compared TAVR with either SAVR or CS, while six compared outcomes across different transcatheter valve platforms. Among the 11 studies comparing TAVR with SAVR or CS, eight reported comparable all-cause mortality between the treatment groups, with no statistically significant differences. One study demonstrated a short-term mortality benefit with TAVR at one year in a low–to–intermediate–risk population (DEDICATE-DZHK6). In addition, the PARTNER 2 SAPIEN 3 cohort reported significantly lower mortality with TAVR at one year; however, this early advantage was not sustained over time, and mortality rates were similar between TAVR and SAVR at five years. Across the six studies comparing different valve platforms, no statistically significant differences in all-cause mortality were observed among balloon-expandable, self-expanding, or mechanically expanded valves. Detailed results are described in the sections below.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Symptomatic Low-Risk Population
In the symptomatic low-risk population, four studies (PARTNER 3, Evolut Low Risk, NOTION, NOTION-2 trial) totaling 1,558 patients treated with TAVR, consistently demonstrated similar outcomes in all-cause mortality between TAVR and SAVR with no statistically significant differences at follow-up times ranging from two to seven years (Leon et al., 2021; Mack et al., 2023; Leon et al., 2025; Forrest et al., 2023; Thyregod et al., 2019; Søndergaard et al., 2019; Jørgensen et al., 2024).
Symptomatic Low or Intermediate-Risk Population
The DEDICATE-DZHK6 trial results favored TAVR over SAVR at one year in all-cause mortality for a mixed-risk group of 701 patients treated with TAVR. Of note, a substantial proportion of patients were enrolled during the COVID-19 pandemic, a period associated with worse outcomes following cardiac surgery. In addition, the trial included a higher proportion of women, and female sex has been known to increase mortality after SAVR (Blankenberg et al., 2024).
Symptomatic Intermediate-Risk Population
In the intermediate-risk group, three RCTs reported no statistically significant difference in all-cause mortality after five year follow-up (PARTNER 2 cohort, Makkar et al., 2020; SURTAVI, Van Mieghem et al., 2022; PARTNER 2 SAPIEN 3 cohort, Madhavan et al., 2023) although the PARTNER 2 SAPIEN 3 observational study observed a statistically significant difference favoring TAVR in one year mortality. One-year mortality in the PARTNER 2 SAPIEN 3 cohort study favored TAVR (Madhavan et al., 2023).
Symptomatic High-Risk Population
The Medtronic Core Valve US High-Risk Pivotal Trial reported 5-year survival rates of 44% for TAVR and 39% for SAVR in the iliofemoral cohort, which included 239 patients at high surgical risk (Arnold et al., 2021).
Symptomatic Women (Across All Risk)
Two analyses involving only female patients yielded no statistically significant differences between TAVR and SAVR in 1-year, all-cause mortality: the RHEIA trial, involving 215 women treated with TAVR (Tchetche et al., 2025) and a post-hoc pooled analysis of the RHEIA trial and the PARTNER 3 trial with 376 women treated with TAVR (Eltchaninoff et al., 2025).
Comparisons of different valve types
Six RCTs reported no statistically significant differences in all-cause mortality, measured in various comparisons of valve platforms (balloon-expandable, self-expanding, and mechanically expanded) at follow-up intervals ranging from 30 days to five years (SOLVE TAVI, CHOICE, SMART, GALILEO, REPRISE III, PORTICO IDE). Most evidence comes from studies directly comparing self-expanding valves (SEV) with balloon-expandable valves (BEV).
Multivariable predictors of mortality
In a multivariable Cox regression analysis evaluating 10-year all-cause mortality, advanced age was the strongest independent predictor of long-term outcomes for AS patients. Elderly age greater than 80 years at baseline was significantly associated with increased mortality risk compared to <80 years of age (Thyregod et al., 2024). In contrast, the type of valve intervention was not independently associated with mortality, with no statistical difference observed for TAVR versus SAVR. Pacemaker implantation at 1-month post-TAVR or SAVR demonstrated a trend toward increased mortality, although this did not reach statistical significance. Male sex and preserved LVEF ≥ 50% at 3-month echocardiographic follow-up were not associated with long-term mortality.
Consistent with these findings, a Cox proportional hazards model reported by Abdel-Wahab et al. (2020) showed that the patient risk profile rather than valve type was associated with shorter survival. In that analysis, female patients had a significantly lower risk of mortality than male patients. Higher baseline surgical risk, as measured by the STS score, was independently associated with an 11% increase in mortality per one unit score increase (p<0.001), as was higher systolic pulmonary artery pressure (p=0.001). Notably, valve type was not associated with mortality in this model, reinforcing that long-term mortality after TAVR is primarily driven by baseline patient characteristics rather than the choice of valve platform.
Conclusion – All-cause mortality in RCTs
All-cause mortality was consistently reported across 11 studies comparing TAVR with standard care (SAVR or CS) and six studies comparing different TAVR valve types. Overall, across the spectrum of surgical risk categories and patient subgroups, TAVR demonstrated comparable all-cause mortality to SAVR, with some early- and mid-term advantages in select subpopulations (e.g., low, low-intermediate, or intermediate risk), but no statistically significant long-term mortality benefit. In symptomatic low-risk populations, mortality results were highly consistent for nine publications across timepoints up to 10 years, reinforcing clinical equipoise for TAVR and SAVR in this group. One trial of mixed low-to-intermediate-risk patients favored TAVR at one year, suggesting a short-term survival advantage. In the intermediate-risk group, studies demonstrated equivalent long-term survival between TAVR and SAVR, with some TAVR benefit at 1-year follow-up in the SAPIEN 3 cohort that was lost at five years. Among high-risk patients in one trial, survival outcomes were again comparable for TAVR and SAVR. Similarly, trials including only female patients, or comparing different transcatheter valve platforms (i.e., BEV, SEV, or MEV), showed no significant difference in early and long-term mortality between interventions. Multivariable analyses consistently indicate that long-term survival after valve replacement is driven predominantly by baseline patient characteristics rather than treatment modality or valve type. Advanced age, female sex, higher surgical risk scores, and elevated pulmonary pressures are the strongest predictors of mortality.
Collectively, these findings support the conclusion that TAVR provides durable survival outcomes comparable to surgery across a wide spectrum of patients, with mortality largely determined by underlying patient risk rather than valve selection. Early mortality advantages observed with TAVR likely reflect its less invasive nature, whereas higher early mortality with SAVR may be related to the procedural burden of sternotomy, cardiopulmonary bypass, and cardiac arrest. Over longer follow-up, survival differences attenuate and become non-significant, potentially reflecting later mortality in the TAVR group, which is associated with higher rates of permanent pacemaker implantation and moderate-to-severe paravalvular regurgitation. These patterns may also be influenced by higher loss to follow-up in the SAVR arm of some studies (e.g., 11.9% in PARTNER), higher prevalence of concomitant procedures during SAVR (e.g., coronary artery bypass grafting) that may improve mid-term surgical outcomes, and the favorable hemodynamic performance and durability of BEVs.
Cardiovascular (CV) mortality
Across the included studies, 13 reported CV mortality outcomes. Of these, 10 studies compared TAVR with SAVR or CS, while three studies focused on comparisons between different valve types. Among the 10 studies comparing TAVR with SAVR or CS, eight reported comparable CV mortality between groups, with no statistically significant differences observed. One trial (DEDICATE-DZHK6) found a statistically significant reduction in 1-year CV mortality with TAVR among low-to-intermediate-risk patients. Another trial (PARTNER 2 SAPIEN 3) showed significantly lower CV mortality with TAVR at one year, though the difference was no longer significant at five years.
No RCT reported results showing worse CV mortality with TAVR compared to SAVR. Furthermore, across the three studies comparing valve platforms, no statistically significant differences in CV mortality were observed among BEV, SEV, or MEV used in TAVR procedures. Detailed results are described in the sections that follow.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Symptomatic Low-Risk Population
In the symptomatic low-risk population, four studies reported CV mortality, all demonstrating comparable outcomes between TAVR and SAVR (Leon et al., 2021; Mack et al., 2023; Leon et al., 2025; Forrest et al., 2022; Thyregod et al., 2019; Sondergaard et al., 2019; Thyregod et al., 2024; Jørgensen et al., 2024). These studies involved 1,558 patients treated with TAVR. In the PARTNER 3 trial, CV mortality was similar between TAVR and SAVR at the 2-year (Leon et al., 2021), 5-year (Mack et al., 2023), and 7-year follow-up (Leon et al., 2025). Consistent shorter-term findings were reported in the Evolut Low Risk trial, with no significant 2-year difference in CV mortality between TAVR and SAVR (Forrest et al., 2022). Longer-term outcomes were also comparable in the NOTION trial, with CV mortality rates of 20.8% for TAVR and 23.0% for SAVR at five years (p = 0.62) (Thyregod et al., 2019) and 49.5% for TAVR and 51.2% for SAVR (p = 0.7) at 10 years (Thyregod et al., 2024). Valve-related deaths also remained low and similar between groups at six years and 10 years (Sondergaard et al., 2019; Thyregod et al., 2024). For low-risk patients aged ≤ 75 years in the NOTION-2 trial, 1-year CV mortality showed no difference between TAVR and SAVR (Jørgensen et al., 2024). Overall, across symptomatic low-risk studies, CV mortality outcomes were comparable between TAVR and SAVR across short-, mid-, and long-term follow-up.
Symptomatic Low or Intermediate-Risk Population
In this mixed-risk group, the DEDICATE-DZHK6 trial demonstrated significantly lower CV mortality among 701 patients treated with TAVR (2.0%) compared to patients treated with SAVR (4.4%) at one year (Blankenberg et al., 2024).
Symptomatic Intermediate-Risk Population
In the intermediate-risk population, three studies reported CV mortality outcomes (Makkar et al., 2020; Madhavan et al., 2023; Van Mieghem et al., 2022; Amrane et al., 2019). As with all-cause mortality, two studies found comparable CV mortality between TAVR and SAVR at five years, for 1,011 TAVR patients in the PARTNER 2 cohort A trial (Makkar et al., 2020) and 864 TAVR patients in the SURTAVI trial (Amrane et al., 2019). In a post hoc cause-of-death analysis from the SURTAVI trial no differences in CV mortality for TAVR or SAVR were observed at 30 days, 120 days, or one year (Amrane et al., 2019), with similar 5-year CV mortality rates of 17.8% for TAVR and 17.4% for SAVR (Van Mieghem et al., 2022). A third study reporting a propensity score-matched analysis of the PARTNER 2 SAPIEN 3 cohort, comprising 783 patients, reported significantly lower 1-year mortality with TAVR compared to SAVR that was not sustained at five years (Madhavan et al., 2023). Collectively, these studies indicate that in intermediate-risk patients, CV mortality is comparable between TAVR and SAVR, with any early differences attenuating over longer-term follow-up.
Symptomatic Women (Across All Risk)
The RHEIA trial examined CV mortality in a population of 215 female patients and reported that 1-year CV mortality was 0.5% in both the TAVR and SAVR-treated groups (Tchetche et al., 2025).
Comparisons of different valve types
Among the included publications comparing transcatheter heart valve systems, CV mortality was reported from three studies (CHOICE, GALILEO, REPRISE III). Across all comparisons, no statistically significant differences in CV mortality were observed between valve platforms, including MEV, SEV, and BEV technologies.
Conclusion – CV Mortality
Across RCTs in symptomatic patients, multiple surgical risk groups, sex-specific analyses, and comparisons of valve platforms, CV mortality outcomes were largely comparable between TAVR and standard management strategies, including SAVR and clinical surveillance. While a small number of publications reported early reductions in CV mortality favoring TAVR, such as at one year or within selected low- or intermediate-risk cohorts, these differences were not consistently sustained over longer-term follow-up. None of the included studies reported higher CV mortality with TAVR than with SAVR or clinical surveillance. Similarly, head-to-head comparisons of transcatheter valve technologies showed no statistically significant differences in CV mortality across MEV, SEV, or BEV platforms. Collectively, these findings indicate that CV mortality outcomes were comparable between TAVR and established treatment strategies and valve platforms across diverse patient populations and follow-up durations.
Stroke
Among the included studies that evaluated all-stroke outcomes, 12 compared TAVR with SAVR or CS, while four compared different transcatheter valve types. Across all 12 studies comparing TAVR with SAVR or CS, stroke rates were comparable between treatment groups, with no statistically significant increase in all-stroke risk associated with TAVR for any patient subgroup. However, three studies examining patients from low- to intermediate-risk populations (PARTNER 3, PARTNER 2 SAPIEN 3 cohort, and the SURTAVI trial) reported a statistically significant reduction in stroke with TAVR compared with SAVR at early follow-up of one to two years, whereas one study reported an increase (NOTION 2 trial). Among trials comparing valve platforms, three studies reported no statistically significant differences in stroke rates among BEVs, SEVs, or MEVs. One exception was the SOLVE TAVI trial, which reported a statistically lower stroke rate with SEVs compared with BEVs at both 30 days and five years, favoring the self-expanding platform. Detailed results are described in the sections below.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Symptomatic Low-Risk Population
In the symptomatic low-risk population, four studies reported stroke outcomes, all of which showed comparable findings between TAVR and SAVR. In the PARTNER 3 trial, a statistically significant reduction in stroke was observed with TAVR compared with SAVR at one year (Leon et al., 2021) that was not sustained at two years (Leon et al., 2021), five years (Mack et al., 2023), or seven years (Leon et al., 2025). Consistent results were observed in the Evolut Low Risk trial, which included 730 TAVR-treated patients and reported similar 2-year all-stroke rates for TAVR and SAVR-treated patients (Forrest et al., 2022). Long-term data from the NOTION trial, showed 5-year stroke rates of 9.0% for TAVR and 7.4% for SAVR (p = 0.65) (Thyregod et al., 2019), a nonsignificant difference that widened between groups at 10 years to 9.7% and 16.4%, respectively, but was not statistically significant (p = 0.1) (Thyregod et al., 2024). An important limitation of these low-risk TAVR trials is that enrolled patients were predominantly in their mid-70s or older, and individuals with bicuspid aortic valves were excluded.
In the NOTION-2 trial, the 1-year stroke rate was significantly higher in the TAVR group (5.4%) than in the SAVR group (1.6%), though statistical estimates were imprecise and reflected a small number of events (Jørgensen et al., 2024). According to study authors, an increased stroke risk in patients undergoing TAVR may be related to excessive valve calcification, greater need for balloon pre- and post-dilation, and more frequent valve repositioning during the procedure, especially in patients with bicuspid valves (Jørgensen et al., 2024). Additionally, a bias in all-stroke diagnosis cannot be excluded in the NOTION 2 trial, as most TAVRs were performed under local anesthesia with immediate hospitalization in the regular ward post-procedurally, rather than cardiac surgery, which was performed under general anesthesia with a minimum 24-hour hospitalization in the intensive care unit. This may have contributed to differential diagnosis of early post-procedural non-disabling stroke.
Symptomatic Low or Intermediate-Risk Population
The DEDICATE-DZHK6 trial, which included 701 mixed low- or intermediate-risk patients treated with TAVR, reported reduced stroke outcomes for TAVR patients compared to SAVR at one year, though the difference was not statistically significant (Blankenberg et al., 2024).
Symptomatic Intermediate-Risk Population
In the symptomatic intermediate-risk population, three studies comparable findings in stroke outcomes between the treatment groups. In the PARTNER 2 cohort A trial and a propensity-matched analysis of the PARTNER 2 SAPIEN 3 cohort, which together included 1,794 patients treated with TAVR, no statistically significant difference between TAVR and SAVR for any stroke was reported at five years (Makkar et al., 2020, Madhavan et al., 2023). The SURTAVI trial, which enrolled 864 patients undergoing TAVR, also demonstrated similar outcomes at five years, with stroke occurring in 11.6% of TAVR patients and 13.6% of SAVR patients (p = 0.16) (Van Mieghem et al., 2022). Of note, both the PARTNER 2 SAPIEN 3 cohort and the SURTAVI trial demonstrated an early reduction in stroke with TAVR compared with SAVR at one and two years, respectively; however, this early advantage attenuated over time, with stroke rates converging and becoming comparable between TAVR and SAVR by 5-year follow-up. A post hoc analysis of SURTAVI further showed that, among survivors at one year, stroke rates were 4.6% in the TAVR group and 5.5% in the SAVR group (Amrane et al., 2019).
Symptomatic Women (Across All Risk)
Two studies reported stroke outcomes for exclusively female patients and demonstrated no statistically significant differences between TAVR and SAVR. The RHEIA trial reported comparable outcomes between treatment groups at one year (Tchetche et al., 2025) consistent with the findings of a pooled analysis of women from the RHEIA and PARTNER 3 trials, which showed a nonsignificant difference in stroke at one year between TAVR and SAVR in women (Eltchaninoff et al., 2025).
Comparisons of different valve types
Among the RCTs, four studies reported all-stroke comparing different transcatheter heart valve systems for TAVR (SOLVE TAVI, GALILEO, CHOICE, REPRISE III). Across these trials, no statistically significant differences in stroke rate were observed among the valve platforms studied, except for one (SOLVE TAVI), which reported that the stroke rate was statistically significantly lower in the SEV group than in the BEV group at 5-year follow-up.
Conclusion - Stroke
Collectively, the evidence consistently demonstrated that stroke rates were comparable between TAVR and SAVR/CS groups, with no statistically significant increase in stroke risk associated with TAVR across any patient subgroup. However, three studies examining patients from low to intermediate risk populations (PARTNER 3, PARTNER 2 SAPIEN 3 cohort, and the SURTAVI trial) reported a statistically significant reduction in stroke for TAVR compared to SAVR at early follow-up of one to two years (Leon et al., 2021; Madhavan et al., 2023; Van Mieghem et al., 2022), while one study reported increased stroke with TAVR (NOTION 2 trial; Jørgensen et al., 2024). Regarding valve platform comparisons, most studies reported no significant differences across MEV, SEV, and BEV systems. However, the SOLVE TAVI trial reported a statistically lower stroke rate with SEV than BEV at both 30 days and five years, findings that were not replicated in other trials.
In summary, across RCT evidence, stroke outcomes following TAVR were consistently comparable to those observed with SAVR or clinical surveillance across risk strata, symptom status, and valve platforms. While a small number of trials reported an early reduction in stroke with TAVR in selected low-to-intermediate-risk populations, these effects were not sustained long-term.
Disabling stroke
Among the included studies that examined disabling stroke, 11 compared TAVR with either SAVR or CS, while three assessed different transcatheter valve types. Across nine of the 11 studies comparing TAVR with SAVR or CS, the rates of disabling stroke were reported to be comparable, with no statistically significant differences observed between the groups. However, two trials, DEDICATE-DZHK6 and PARTNER 2 SAPIEN 3, reported a statistically significant reduction in disabling stroke, favoring TAVR at 1-year and 5-year follow-up, respectively. Among the studies comparing valve types, two trials reported no differences in disabling stroke between BEVs and SEVs. However, one trial, REPRISE III, demonstrated a significantly lower disabling stroke rate with the MEV at one, two, and five years of follow-up, favoring MEV over SEV. Detailed results are described in the sections below.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Symptomatic Low-Risk Population
In the symptomatic low-risk population, all four studies that examined disabling stroke outcomes reported no statistically significant differences between TAVR and SAVR. At one year after treatment, the NOTION-2 trial, including 187 TAVR patients, reported no significant difference in disabling stroke between patients receiving TAVR or SAVR (Jørgensen et al., 2024). In the PARTNER 3 trial, which included 496 patients treated with TAVR, the incidence of disabling stroke was low and did not significantly differ between groups at 2-, 5-, and 7-year follow-up (range 0.85% to 5.1% for TAVR patients at two and seven years) (Leon et al., 2021; Mack et al., 2023; Leon et al., 2025). Similar findings were reported for the 730 TAVR patients included in the Evolut Low Risk Trial, where disabling stroke was comparable between interventions and occurred in 1.5% and 2.9% of TAVR patients and 2.7% and 3.8% of SAVR patients at two and four years, respectively (Forrest et al., 2022; Forrest et al., 2023). Long-term data from the NOTION trial, which treated 145 TAVR patients, showed that “stroke with sequelae” (used as a proxy for disabling stroke) occurred in 6.9% of TAVR patients and 10.4% of SAVR patients at 10 years, with no significant difference between groups (Thyregod et al., 2024).
Symptomatic Low or Intermediate-Risk Population
In this mixed-risk group, one publication reported disabling stroke among 701 patients treated with TAVR, with results favoring TAVR over SAVR at one year. The DEDICATE-DZHK6 trial reported that at one year, disabling stroke was 1.3% for TAVR and 3.1% for SAVR. One possible explanation is that a substantial proportion of patients were enrolled during the COVID-19 pandemic, a period associated with worse outcomes following cardiac surgery, resulting in a higher frequency of stroke rate in the SAVR group (Blankenberg et al., 2024).
Symptomatic Intermediate-Risk Population
In the intermediate-risk population, three studies reported disabling stroke outcomes. Of these, one favored TAVR, while the other two reported comparable outcomes between TAVR and SAVR. A propensity score-matched analysis of the PARTNER 2 SAPIEN 3 cohort (783 patients per group) reported a statistically significant reduction in disabling stroke with TAVR at five years, with 5.8% in the TAVR group versus 7.9% in the SAVR group (Madhavan et al., 2023). As reported above, although 5-year all-stroke rates were similar between the SAVR and TAVR groups, disabling stroke was less frequent with TAVR. The early reduction in disabling stroke observed with TAVR persisted through 5-year follow-up and was driven by events occurring early in the SAVR group, with no additional differences between one and five years. In contrast, nondisabling strokes occurring after the first year were more frequent in the TAVR group, with the underlying mechanism remaining unclear (Madhavan et al., 2023).
In contrast, in the PARTNER 2 Cohort A trial, which included 1,011 patients treated with TAVR, as well as the SURTAVI trial, which enrolled 864 patients in the TAVR arm, there was no significant difference in the 5-year incidence of disabling stroke between the TAVR and SAVR groups (Makkar et al., 2020; Van Mieghem et al., 2022). A post hoc analysis of 1-year survivors in SURTAVI further showed disabling stroke rates of 1.4% in the TAVR group and 2.0% in the SAVR group, although no p-value was reported (Amrane et al., 2019).
Symptomatic Women (Across All Risk)
In a specific population of female patients, the RHEIA trial examined disabling stroke and reported comparable outcomes between TAVR and SAVR where at one year, disabling stroke was 0.9% in the TAVR group and 1.5% in the SAVR group, with no statistically significant rate difference (Tchetche et al., 2025).
Comparisons of different valve types
Among the included studies comparing transcatheter heart valve systems, disabling stroke outcomes were reported in three studies. Across two studies (SMART, PORTICO IDE), there were no statistically significant differences in disabling stroke between SEV and BEV. However, the REPRISE III trial reported a statistically significant reduction in disabling stroke with MEV compared to SEV devices.
Conclusion – Disabling Stroke
RCTs in symptomatic patients with severe AS, across multiple surgical risk strata, sex-specific analyses, and comparisons of valve platforms, demonstrated that disabling stroke outcomes occurred with low frequency and were largely comparable between TAVR and standard management strategies, including SAVR and clinical surveillance. Only two studies of a mixed low-to-intermediate risk population (DEDICATE-DZHK6) and an intermediate-risk population (a propensity score-matched analysis of the PARTNER 2 SAPIEN 3 cohort), reported disabling stroke results which favored TAVR over SAVR at one and five years, respectively. Findings for symptomatic low-risk, and most intermediate-risk patients, as well as female-only cohorts, showed comparable disabling stroke outcomes between intervention groups. In valve technology comparisons, most RCTs reported no significant differences in disabling stroke outcomes between SEV and BEV platforms. However, the REPRISE III trial showed a statistically significant advantage of MEV over SEV in the high-risk population at all follow-up points up to five years. Collectively, these findings indicate that disabling stroke outcomes were comparable between TAVR and established treatment strategies across all risk strata and populations studied. Additionally, among valve platforms, the MEV system may offer some advantages, though further research may be warranted to confirm this finding in broader populations.
New permanent pacemaker implantation
Among the included studies that evaluated new permanent pacemaker implantation after TAVR procedures 12 studies compared TAVR with either SAVR or CS, while five compared different valve types. Across the 12 studies comparing TAVR with SAVR or CS, four reported comparable rates of new permanent pacemaker implantation between the two groups, with no statistically significant difference. However, eight studies reported a significantly higher rate of new pacemaker implantation (excluding patients with pre-existing pacemakers or Implantable Cardioverter-Defibrillator [ICD] devices at baseline) in the TAVR group than in the SAVR group, with follow-up durations ranging from one to 10 years.
Among the five studies that compared valve types, mixed data were observed across devices. The REPRISE III trial demonstrated that MEV was associated with a statistically higher rate of pacemaker implantation than SEV at one, two, and five years of follow-up. The CHOICE trial and PORTICO IDE trial reported a significantly higher pacemaker implantation rate with SEV compared with BEV at 30-day and 1-year follow-up. Two additional trials observed numerically higher pacemaker rates with SEV compared with BEV across follow-up periods ranging from 30 days to five years, although these differences did not reach statistical significance. Detailed results are described in the sections below.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Symptomatic Low-Risk Population
In the symptomatic low-risk group, four studies included pacemaker outcomes with three demonstrating statistically significantly higher pacemaker implantation rates in the TAVR group than in the SAVR group, while one demonstrated comparable results.
For short-term outcomes at one year in the NOTION-2 trial, pacemaker implantation was approximately doubled for TAVR compared to SAVR patients (excluding those with baseline devices) (Jørgensen et al., 2024). The Evolut Low Risk trial, which included 730 patients treated with TAVR, also reported substantially higher pacemaker implantation rates (excluding those with baseline pacemakers) in the TAVR group (21.8%) than in the SAVR group (8.2%) at two years, yielding a between-group difference of 13.6% (Forrest et al., 2022) that persisted with similar group-level frequencies at four years (Forrest et al., 2023). A stronger trend was observed in the NOTION trial, where 41.7% of TAVR patients required a new pacemaker (excluding those with baseline pacemakers) at five years compared to 7.8% in the SAVR group (p < 0.001) (Thyregod et al., 2019). These results again remained comparable at longer follow-up, with significantly higher pacemaker implantation rates remaining for TAVR versus SAVR patients at 10 years (Thyregod et al., 2024).
In contrast, in the PARTNER 3 trial, which included 496 patients treated with TAVR, no statistically significant differences were observed between TAVR and SAVR in pacemaker implantation (excluding those with baseline pacemakers) at multiple timepoints of two (Leon et al., 2021), five (Mack et al., 2023), and seven years (Leon et al., 2025), with lower reported proportions of TAVR patients with pacemaker implantation at two years than the other trials for this risk group.
Symptomatic Low or Intermediate-Risk Population
In the symptomatic low- or intermediate-risk population, pacemaker outcomes were reported in one publication from a single study. The DEDICATE-DZHK6 trial, which treated 701 patients with TAVR, found a nearly doubled pacemaker implantation rate in the TAVR group (11.8%) compared to the SAVR group (6.7%) at one year, indicating a statistically significant disadvantage for pacemaker placement for TAVR compared to SAVR (Blankenberg et al., 2024).
Symptomatic Intermediate-Risk Population
In the symptomatic intermediate-risk population, three publications from three studies reported pacemaker outcomes. Two studies showed higher pacemaker implantation rates with TAVR, while one showed no statistically significant difference. The propensity score-matched analysis of the PARTNER 2 SAPIEN 3 cohort reported a statistically significantly higher 5-year rate of pacemaker implantation with TAVR (Madhavan et al., 2023) that was also demonstrated in the SURTAVI trial, which reported a markedly higher 5-year pacemaker implantation rate (excluding baseline devices) in the TAVR group (39.1%) compared to the SAVR group (15.1%), favoring SAVR (Van Mieghem et al., 2022). In contrast, the PARTNER 2 Cohort A trial, which included 1,011 TAVR patients, reported comparable 5-year pacemaker rates of 15.5% for TAVR and 13.0% for SAVR (Makkar et al., 2020).
Symptomatic Women (Across All Risk)
In the subgroup of symptomatic women across all risk categories, mixed pacemaker outcomes were reported in two publications. The RHEIA trial found a significantly higher 1-year pacemaker rate in the TAVR group (8.8%) than in the SAVR group (2.9%) (Tchetche et al., 2025), while a pooled analysis of women from the RHEIA and PARTNER 3 trials showed a non-significant 1-year difference of 1.8%, suggesting a comparable rate between TAVR and SAVR in this overlapping patient population (Eltchaninoff et al., 2025).
Comparisons of different valve types
Among studies comparing valve platforms, the MEV (Lotus) had the highest pacemaker implantation rate compared to SEV at 30 days, one year, two years, and five years in the REPRISE III trial. When comparing SEVs to BEVs, results were more mixed, with numerically higher implantation rates with SEV that did not always reach statistical significance across trials. When SEV was compared to a group of CAVs, of which 65.7% were BEVs, the 30-day rate of pacemaker implantation was significantly higher for the Portico valve group (27.7%) compared to the CAV group (11.6%) (PORTICO IDE).
Conclusion – New Permanent Pacemaker Implantation
Twelve studies compared TAVR with either SAVR or CS, and five compared different transcatheter valve types for the outcome of new permanent pacemaker implantation. Overall, the evidence indicates that, among patients without pacemakers at baseline, TAVR was associated with a higher risk of permanent pacemaker implantation compared to SAVR. Though results were mixed in terms of statistical significance for low-and intermediate-risk patients, trials commonly demonstrated higher periprocedural pacemaker rates with TAVR verses SAVR up to long-term follow-up of 10 years. Among symptomatic women with AS, the RHEIA trial showed a higher 1-year rate with TAVR, but this was not supported in a pooled analysis of RHEIA and PARTNER 3 trials, suggesting potential variability by study design or population size. Among studies comparing valve platforms, the MEV (Lotus) had the highest pacemaker implantation rate compared to SEV at 30 days, one year, two years, and five years in the REPRISE III trial. When comparing SEVs to BEVs, results were more mixed, with numerically higher implantation rates with SEV that did not always reach statistical significance across trials.
The primary reason for the higher pacemaker requirement in TAVR is procedure-related conduction disturbances, including new-onset left bundle-branch block and advanced atrioventricular block (Moradi et al., 2025). These disturbances often result from direct injury to the cardiac conduction system during transcatheter procedures (Kazemian et al., 2024). Predictors of the need for a pacemaker include pre-existing conduction abnormalities and specific anatomical factors that are often beyond the operator's control (Kazemian et al., 2024). However, the adoption of specialized implantation techniques, such as the "cusp-overlap" technique, could reduce the incidence of new permanent pacemaker implantations in the future by optimizing valve positioning (Forrest et al., 2022). Newer-generation valves, such as the SAPIEN 3 and Evolut R/PRO, may reduce the incidence of pacemaker implantation by more than one-third compared to older device generations (Kazemian et al., 2024).
Myocardial infarction (MI)
Among the studies that evaluated MI, 11 compared TAVR with either SAVR or CS, and four compared different valve types with respect to MI. Across the 11 studies comparing TAVR with SAVR/CS, MI rates were comparable between treatment groups, with no statistically significant differences reported. Similarly, across the four studies that evaluated different transcatheter valve platforms, including balloon-expandable, self-expanding, and mechanically expanded valves, no statistically significant differences in MI incidence were observed. An exception was the SOLVE TAVI trial, which reported a significantly lower incidence of MI with SEVs compared with BEVs at five years of follow-up. Detailed results are described in the sections below.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Symptomatic low-risk population
In the symptomatic low-risk population, four studies demonstrated neutral findings in MI outcomes. In the PARTNER 3 trial, there was no statistically significant difference between TAVR and SAVR for MI at two years (Leon et al., 2021) or at extended follow-up of five years (Mack et al., 2023) or seven years (Leon et al., 2025). Similarly, the NOTION-2 and Evolut Low Risk trials reported comparable 1-year (Jørgensen et al., 2024) and 2-year (Forrest et al., 2022) MI outcomes for the TAVR and SAVR groups. MI rates were higher at longer-term follow-up in the NOTION trial, with 5-year MI rates of 7.7% for TAVR and 7.4% for SAVR (Thyregod et al., 2019), and 10-year rates of 11.0% and 8.2%, respectively (Thyregod et al., 2024), though these differences were not statistically significant.
Symptomatic low- or intermediate-risk population
In the symptomatic low- or intermediate-risk population, one publication from a single study reported MI outcomes, with comparable findings. The DEDICATE-DZHK6 trial, reported 1-year MI rates of 1.0% for TAVR and 2.1% for SAVR (Blankenberg et al., 2024).
Symptomatic intermediate-risk population
In the symptomatic intermediate-risk population, two studies demonstrated neutral results in MI outcomes. The PARTNER 2 cohort A trial, which treated 1,011 patients with TAVR, reported comparable results between TAVR and SAVR at two years and at five years (Makkar et al., 2020). These findings were consistent with those shown in the SURTAVI trial for 864 TAVR patients at five years (Van Mieghem et al., 2022). A post hoc analysis of the SURTAVI study further reported that, among survivors at one year, MI rates remained similarly low at 1.3% for TAVR and 0.9% for SAVR (Amrane et al., 2019).
Symptomatic women (Across All Risk)
In symptomatic women across all risk categories, two studies demonstrated comparable findings in MI outcomes between TAVR and SAVR. The RHEIA trial reported a 1-year MI rate of 0.0% for TAVR and 1.0% for SAVR (Tchetche et al., 2025) and the MI outcome estimates were slightly higher in a pooled analysis from the RHEIA and PARTNER 3 trials, which reported 30-day MI rates of 0.3% in the TAVR group and 1.5% in the SAVR comparison group (Eltchaninoff et al., 2025).
Comparisons of different valve types
Among the RCTs, four studies reported MI comparing different transcatheter heart valve systems for TAVR. Most studies reported no statistically significant differences in MI among the valve platforms studied (e.g., BEV, SEV, or MEV), except one (SOLVE TAVI), which reported that patients who received SEV had a lower MI rate than those receiving BEV. Most evidence comes from studies directly comparing SEV with BEV.
Conclusion - MI
Across RCTs comparing TAVR with SAVR or CS, the risk of MI remained consistently low and comparable across treatment arms. Eleven studies compared TAVR with SAVR or CS, and four compared different valve types.
In comparisons between TAVR and SAVR or CS, all patient subgroups, including symptomatic low-risk, intermediate-risk, and mixed-risk populations, showed comparable MI rates across interventions. Most studies reported either no significant difference or low absolute event rates, which limited the ability to draw definitive conclusions. Even in studies with long-term follow-up (e.g., PARTNER 3 at seven years, NOTION at 10 years), MI rates between TAVR and SAVR remained similar. Overall, the evidence suggested that TAVR does not increase the risk of MI compared with surgical or conservative approaches, even with extended follow-up. In head-to-head comparisons of valve platforms, findings were largely consistent with the above. Trials comparing SEV, BEV, and MEV generally showed no statistically significant differences in MI rates. The SOLVE TAVI trial was the only exception, reporting a significantly lower MI incidence with SEV compared to BEV at five years that was not replicated in other large-scale analyses.
In conclusion, current evidence from randomized trials indicates that the incidence of MI following TAVR is low and comparable to that following SAVR or CS across a range of surgical risk profiles. Valve selection also does not appear to significantly influence MI risk, though isolated findings, such as those from the SOLVE TAVI trial, may warrant further investigation.
Reintervention
Among the included studies, nine compared TAVR with either SAVR or CS, and two compared different valve types. Across the nine studies comparing TAVR with SAVR or CS, seven reported comparable reintervention rates with no statistically significant differences. However, two studies conducted in intermediate-risk populations (PARTNER 2 and SURTAVI) found significantly higher reintervention rates associated with TAVR. Among valve comparison trials, one study found no statistically significant difference in reintervention rates between BEV and SEV. In contrast, the REPRISE III trial reported a statistically higher reintervention rate with SEV at both 1- and 2-year follow-up, favoring MEV over SEV, though the groups subsequently showed comparable reintervention rates at five years. Detailed results are described in the sections below.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Among nine studies comparing TAVR with SAVR or CS for aortic valve reintervention, seven reported neutral findings, while two reported significantly higher reintervention rates with TAVR. No study provided results that favored TAVR for this endpoint.
Symptomatic Low-Risk Population
In the symptomatic low-risk population, four studies consistently demonstrated neutral results (Thiele et al., 2021; Mack et al., 2023; Leon et al., 2025; Forrest et al., 2022; Forrest et al., 2023; Sondergaard et al., 2019; Thyregod et al., 2019; Thyregod et al., 2024; Jørgensen et al., 2024). In the PARTNER 3 trial, reintervention rates were similarly low between groups at two years (0.8% vs. 0.9%, p = 0.85), and at 5- and 7-year follow-up. The Evolut Low Risk trial also showed no difference between groups at two years, and reinterventions remained infrequent at 4-year follow-up (1.3% for TAVR vs. 1.7% for SAVR). Similarly, the NOTION trial reported non-significant differences at five, six, and 10 years (Sondergaard et al., 2019; Thyregod et al., 2019; Thyregod et al., 2024), and comparable 1-year reinterventions in NOTION-2 of 1.1% for TAVR and 2.2% for SAVR (Jørgensen et al., 2024).
Symptomatic Low or Intermediate-Risk Population
In the symptomatic low- or intermediate-risk population, the DEDICATE-DZHK6 trial (Blankenberg et al., 2024) reported no significant difference in the risk of reintervention between TAVR and SAVR at one year.
Symptomatic Intermediate-Risk Population
In the symptomatic intermediate-risk population, three studies showed mixed results (Makkar et al., 2020; Madhavan et al., 2023; Van Mieghem et al., 2022; Amrane et al., 2019). Two studies reported findings indicating a significantly higher risk of reintervention after TAVR. The PARTNER 2 cohort A trial showed a 5-year hazard ratio of 3.28, significantly favoring SAVR for reduced risk of aortic valve reintervention (Makkar et al., 2020). After TAVR, reinterventions were primarily due to progressive stenosis (10/21) or aortic regurgitation (11/21), with most patients managed by repeat TAVR or balloon valvuloplasty. In contrast, reinterventions after surgery were mainly due to endocarditis (4/6) and were usually treated with repeat surgery. The in-hospital mortality was markedly higher in the surgical group (50% vs. 5% with TAVR) (Makkar et al., 2020).
Similarly, the SURTAVI trial showed over double the risk of reintervention at five years in the TAVR group than with surgery, primarily driven by a greater number of early reinterventions after TAVR. Reintervention rates between two and five years were similarly low for both approaches (Van Mieghem et al., 2022). A post hoc analysis of SURTAVI further showed that, among survivors at one year, reintervention rates were 1.9% in the TAVR group and 0.1% in the SAVR group (p = NR) (Amrane et al., 2019). A propensity score-matched analysis of the SAPIEN 3 cohort also reported comparable reintervention outcomes between TAVR and SAVR (Madhavan et al., 2023).
Comparisons of different valve types
Among the RCTs, two studies reported reintervention comparing different transcatheter heart valve systems for TAVR. Findings across both trials suggested generally low reintervention rates across valve platforms, with some potential advantage observed for MEV over SEV at 1- and 2-year follow-up in the REPRISE III trial.
Conclusion - Reintervention
Among the included studies reporting on reintervention outcomes, nine compared TAVR with either SAVR or CS, and two compared different transcatheter valve types. Across the nine studies evaluating TAVR versus SAVR or CS, the majority reported comparable findings, suggesting no significant difference in reintervention rates. No study in this comparison favored TAVR over surgery for reintervention outcomes. In asymptomatic and low-risk symptomatic populations, including trials such as Evolut Low Risk, PARTNER 3, NOTION, and NOTION-2, reintervention rates were low and comparable between TAVR and SAVR across various follow-up durations (up to 10 years). These findings support the durability of TAVR in lower-risk patients. In intermediate-risk populations, findings were more variable, with two studies in intermediate-risk populations (PARTNER 2 and SURTAVI) reporting significantly higher reintervention rates with TAVR, raising concerns about long-term durability in this subgroup.
For valve-to-valve comparisons, the REPRISE III trial (MEV vs SEV) showed consistently lower reintervention rates with the MEV (Lotus valve) with statistically significant results at one and two years, though the 5-year difference did not reach statistical significance. This suggests a potential durability advantage for MEV in high-risk patients at 1- and 2-year follow-up. Conversely, the SMART trial comparing SEV and BEV in patients with small annuli reported low and similar reintervention rates across the overall population and among women, with no statistically significant differences. These findings support the procedural safety of both platforms in anatomically challenging cases.
While most RCTs report comparable reintervention rates between TAVR and SAVR, the increased rates observed in intermediate-risk patients underscore the need for careful valve selection and long-term surveillance in this category of patients. Among valve types, MEV may offer an advantage over SEV, while BEV and SEV perform similarly in small annuli populations.
Patient-reported outcomes (PROs): Kansas City Cardiomyopathy Questionnaire (KCCQ)
Among the studies that reported on PROs using the KCCQ, 10 compared TAVR with either SAVR or CS, while three compared different valve types. The KCCQ is a 23-item questionnaire and includes items about daily functioning, symptoms, and quality of life. KCCQ values range from 0 to 100; higher scores indicate better health status, and changes of five, 10, and 20 points indicate small, moderate, and large improvements, respectively. Across the 10 studies comparing TAVR with SAVR or CS, TAVR consistently showed greater improvement in health status at early time points, particularly within the first month following the procedure. Over the longer term, PROs were generally comparable between TAVR and SAVR, with no statistically significant differences observed. Among the three studies comparing valve types, two found no significant differences in KCCQ outcomes across valve platforms. However, the SMART trial reported that SEV was associated with significantly greater improvement in KCCQ scores at one year follow-up compared with BEV (Arnold et al., 2021; Herrmann et al., 2024; Tchétché et al., 2024). Detailed results are described in the sections below.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Symptomatic Low-Risk Population
Three studies reported KCCQ outcomes in the symptomatic low-risk population. Early time points favored TAVR, while later follow-up showed comparable results. The NOTION-2 trial (187 TAVR patients) showed that KCCQ improved from baseline to one month in 16% of TAVR patients versus 4% of SAVR patients (Jørgensen et al., 2024), though by one year, improvement was comparable and was reported in 17% of patients in both groups (Jørgensen et al., 2024). Similarly, in the PARTNER 3 trial, the 1-month KCCQ overall summary scores were significantly higher for TAVR (88.9) than SAVR (72.8) (Leon et al., 2021). This difference persisted at two years, with mean scores of 89.5 for TAVR and 87.9 for SAVR reflecting a small but significant difference between groups (Leon et al., 2021). At five and seven years, the scores were nearly identical, suggesting that health status findings were similar in the two groups over time (Mack et al., 2023; Leon et al., 2025). Of note, missing KCCQ-OS score data could not be fully accounted for with multiple imputation in this publication. The Evolut Low Risk Trial (730 TAVR patients) also reported similar 2-year changes from baseline: 20.9 points for TAVR vs. 20.1 for SAVR (Forrest et al., 2022).
Symptomatic Intermediate-Risk Population
In intermediate-risk patients, two studies showed similar 5-year KCCQ outcomes between TAVR and SAVR. The PARTNER 2 cohort A trial (1,011 TAVR patients) showed mean increases from baseline of 19.6 points for TAVR and 20.5 points for SAVR (Makkar et al., 2020). Similarly, the SURTAVI trial (864 TAVR patients) reported a 5-year gain of 15.3 points for TAVR and 14.3 points for SAVR (Van Mieghem et al., 2022). These results indicate similar long-term improvements in health status with both procedures.
Symptomatic High-Risk Population
The US High-Risk Pivotal Trial evaluated health status outcomes using the KCCQ and found early advantages with TAVR that diminished over time. In the iliofemoral TAVR cohort (331 patients), the mean KCCQ improvement at one month was 16.8 points higher with TAVR than with SAVR, indicating a substantial early benefit (Arnold et al., 2021). However, this difference had narrowed to 1.8 points by six months and remained small and non-significant at five years (1.7 points), reflecting comparable and sustained long-term health status between groups. In the non-iliofemoral cohort (64 patients), no significant differences in KCCQ scores were observed at any timepoint (one month through five years) (Arnold et al., 2021). These findings suggest that while TAVR may offer faster early recovery in select high-risk patients, long-term health status outcomes are similar between TAVR and SAVR.
Symptomatic Women (Across All Risk)
The RHEIA trial and the pooled analysis from RHEAI and PARTNER both favored TAVR for early recovery of 30 days. In the RHEIA trial, the KCCQ score improvement at 30 days was significantly greater with TAVR, with a mean difference of 8.78 points (Tchetche et al., 2025) that was reduced to 2.46 points and no longer statistically significant at one year (Tchetche et al., 2025). Similar 30-day and 1-year KCCQ scores were observed in the pooled analysis, though the results significantly favored the TAVR group at both time points in this larger patient sample (Eltchaninoff et al., 2025). A favorable outcome at one year (defined as survival with KCCQ ≥75 and no decline of >10 points) was achieved in 78.2% of TAVR patients compared with 73.0% in the SAVR group (Eltchaninoff et al., 2025). These findings suggest that while short-term health status benefits with TAVR are significant, differences narrowed over time.
Comparisons of different valve types
Among the RCTs, three studies reported health status comparing different transcatheter heart valve systems for TAVR. The SMART trial found that SEV was associated with significantly greater improvements in KCCQ at one year than BEV, both in the overall population and among women. Conversely, the PORTICO IDE trial demonstrated comparable 1-year KCCQ scores between the Portico valve (a self-expanding system) and commercially available valves, most of which were balloon-expandable. Finally, the REPRISE III trial, which compared MEVs with SEVs, reported no significant differences in health status outcomes at any time point up to five years.
Minimum Clinically Important Difference (MCID)
Disease-specific health status as assessed from the patient's perspective with the KCCQ consists of 23 questions addressing five health domains pertaining to heart failure: symptoms, physical limitation, social limitation, self-efficacy, and quality of life. These individual scales are combined into an overall summary scale with values ranging from 0 to 100; higher scores indicate fewer symptoms and better quality of life. Previous studies have suggested that KCCQ summary scores correlate roughly with NYHA functional class as follows: class I is roughly equal to KCCQ summary score of 75 to 100; class II, to a score of 60 to 74; class III, to a score of 45 to 59; and class IV, to a score of 0 to 44.17 The KCCQ has undergone extensive validation and has been shown to independently predict mortality and healthcare costs in heart failure populations (Reynolds et al., 2011). A change of five points is considered to be a small but clinically important change, whereas changes of 10 and 20 points are considered moderate-to-large and large-to-very large clinical changes (Spertus et al., 2020).
Conclusion – PROs
Ten studies evaluated PROs using the KCCQ by comparing TAVR with either SAVR or CS and an additional three compared different transcatheter valve types. When comparing TAVR to SAVR or CS, results consistently demonstrated greater improvement in health status with TAVR at early time points, particularly within the first month after the procedure. These early gains were observed across risk groups, low-risk, high-risk, and female-specific cohorts, and were statistically significant in several trials. However, over longer-term follow-up (≥5 years), the magnitude of benefit generally declined, with KCCQ scores converging between TAVR and SAVR in nearly all trials. This trend was consistent in the intermediate-risk population as well, where both PARTNER 2 and SURTAVI reported nearly identical long-term KCCQ gains in both TAVR and SAVR arms. These findings suggest that, while TAVR may lead to more rapid recovery and early improvements in quality of life, long-term PROs are largely comparable to those achieved with surgery.
In comparisons between valve types, the evidence was mixed but suggested that among transcatheter valve platforms, SEVs may offer better short-term quality-of-life gains than BEVs in certain subgroups.
The early health status advantage of TAVR was primarily attributed to its less invasive nature, which avoids the clinical trauma associated with a full sternotomy, cardiac arrest, and the use of cardiopulmonary bypass (Pascoal et al., 2026). These procedural differences result in shorter hospital lengths of stay and a significantly higher likelihood of discharge home rather than to a rehabilitation facility (Forrest et al., 2022). Over the longer term, the initial disparity in health status between the two interventions diminished as surgical patients fully recovered from the procedural trauma of open-heart surgery, and by the 6-month to 1-year follow-up, patients in both groups typically reached a similar level of clinical and functional improvement (Arnold et al, 2021). At extended follow-up intervals ranging from five to seven years, KCCQ-OS scores remained high and were maintained at statistically comparable levels between TAVR and surgery. Additionally, potential long-term complications associated with TAVR, such as increased rates of permanent pacemaker implantation or paravalvular leak, may counterbalance the initial recovery benefits, leading to late outcomes that align with those of surgery (Arnold et al, 2021). This evidence may help to weigh the procedural choices, particularly in populations where early recovery and patient experience are priorities.
Composite of all-cause death, all stroke (disabling or non-disabling), or rehospitalization
Seven studies reported data on a composite outcome of all-cause death, stroke, or rehospitalization, and all compared TAVR with either SAVR or CS. TAVR was consistently associated with early benefits, particularly in low-risk and female populations, though these benefits mostly attenuated over longer-term follow-up. No studies comparing different valve platforms evaluated this composite endpoint. Notably, the definitions of rehospitalization varied across studies. The PARTNER 3, RHEIA, and NOTION-2 trials specified rehospitalization due to valve-related, procedural, or heart failure issues (Thiele et al., 2021; Jørgensen et al., 2024; Tchetche et al., 2025). The PARTNER 2 trial applied a broader definition, which was refined in secondary endpoints to specify worsening heart failure or valve-related events (Makkar et al., 2020). Detailed results are described in the sections below.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Symptomatic Low-Risk Population
Three randomized trials reported this composite outcome in the symptomatic low-risk group. One trial demonstrated sustained benefit for TAVR at four years (with 18.0% and 22.4% of TAVR and SAVR patients having this outcome, respectively; Forrest et al., 2023); another showed neutral outcomes at one year (10.2% for TAVR and 7.1% for SAVR; Jørgensen et al., 2024); and the third favored TAVR at one and two years but reported comparably higher outcome risk at five and seven years of follow-up (the PARTNER 3 trial; Leon et al., 2021, Mack et al., 2023, Leon et al., 2025).
Symptomatic Intermediate-Risk Population
Two intermediate-risk studies reported mixed results. A propensity score-matched analysis of the SAPIEN 3 cohort (783 TAVR patients) showed a 1-year composite rate of 18.4% for TAVR vs. 27.2% for SAVR, favoring TAVR (Madhavan et al., 2023) that was neutral at five years (Madhavan et al., 2023). Conversely, the PARTNER 2 Cohort A trial (1,011 TAVR patients) reported a 5-year composite rate of 61.8% for TAVR compared to 53.5% for SAVR, indicating statistically significant results against TAVR (Makkar et al., 2020).
Symptomatic Women (Across All Risk)
One trial and one pooled analysis reported this composite among symptomatic women, both favoring TAVR. In the RHEIA trial the 1-year event rate was 8.9% for TAVR vs. 15.6% for SAVR (Tchetche et al., 2025), with a significant absolute difference between groups that was similar to those observed in a patient-level pooled analysis from RHEIA and PARTNER 3 (376 TAVR patients) at one year: 8.5% for TAVR vs. 16.8% for SAVR (Eltchaninoff et al., 2025).
Comparisons of different valve types
No publication reported the composite endpoint of death, stroke, or hospitalization, comparing different transcatheter heart valve systems for TAVR.
Conclusion – Composite of all-cause death, all stroke (disabling or non-disabling), or rehospitalization
Across seven studies reporting the composite outcome of all-cause death, stroke, or rehospitalization, TAVR was consistently associated with early benefits in low-risk and female populations; these benefits attenuated over longer-term follow-up. No studies comparing different valve platforms evaluated this composite endpoint.
Among the symptomatic low-risk patient group, early outcomes at one to two years significantly favored TAVR over SAVR, though trials with long-term follow-up at five and seven years showed attenuation of this benefit. The NOTION-2 trial showed no difference between groups at one year, reflecting possible equipoise in younger, low-risk patients. TAVR was associated with significantly better outcomes at one year in both the RHEIA trial and the pooled analysis with PARTNER 3, suggesting a consistent benefit in female patients across risk groups.
Among the symptomatic intermediate-risk patients, the evidence was mixed. While a propensity score-matched analysis of SAPIEN 3 demonstrated early benefit at one year, this advantage disappeared by five years. Conversely, the PARTNER 2 Cohort A trial showed higher composite event rates with TAVR at five years, favoring SAVR. Notably, definitions of rehospitalization varied across studies, ranging from broad CV causes to more specific valve-related or heart failure events, thereby affecting comparability and the interpretation of results.
Composite of all-cause mortality or disabling stroke
Among the studies that evaluated the composite outcome of all-cause mortality or disabling stroke, 10 compared TAVR with either SAVR or CS, while two compared different valve types. Across the 10 studies comparing TAVR with SAVR or CS, findings were mixed. In low-risk populations, the PARTNER 3 trial showed early benefit favoring TAVR at one year, but by seven years, outcomes were comparable. The Evolut Low Risk trial reported comparable outcomes between interventions at two years, with a benefit favoring TAVR at four years. In low-to-intermediate-risk patients, the DEDICATE-DZHK6 trial showed significantly better outcomes with TAVR at 1-year follow-up. In intermediate-risk populations, the SAPIEN 3 cohort demonstrated a benefit at one year, favoring TAVR, but outcomes were again comparable at five years. The remaining six studies showed no statistically significant differences in this composite outcome between TAVR and SAVR.
Among the two studies that compared valve platforms, the PORTICO IDE trial found no significant differences in the composite outcome between the Portico SEV and a mixed group of commercially available valves at one and two years. However, the REPRISE III trial reported that the MEV was associated with lower event rates at one and two years compared to the SEV, although by five years, outcomes were similar. Detailed results are described in the sections below.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Symptomatic Low-Risk Population
In the symptomatic low-risk population, three randomized studies assessed the composite endpoint of all-cause death or disabling stroke. The PARTNER 3 trial (496 TAVR patients) demonstrated a significant early benefit for TAVR, with a 1-year event rate of 1.0% compared to 3.1% for SAVR (Thiele et al., 2021). However, this advantage diminished over time as the number of composite outcome events increased: rates were 3.1% for TAVR versus 3.8% for SAVR at two years, 11.5% and 9.8% at five years, respectively (Mack et al., 2023), and 21.7% versus 16.8% at seven years, respectively, though the difference was not statistically significant (Leon et al., 2025).
The Evolut Low Risk Trial (730 TAVR patients) found TAVR to be noninferior to surgery at two years, with event rates of 4.3% for TAVR and 6.3% for SAVR (Forrest et al., 2022). Over time, the benefit appeared to increase, with a 26% relative reduction in the hazard of death or disabling stroke through four years that favored TAVR (Forrest et al., 2023). Finally, the NOTION-2 trial (187 TAVR patients) enrolled younger, low-risk patients (aged ≤75 years) and found comparable 1-year outcomes between TAVR and SAVR, with no significant difference for this endpoint (Jørgensen et al., 2024).
Symptomatic Low or Intermediate-Risk Population
In the symptomatic low- or intermediate-risk group, the DEDICATE-DZHK6 trial (701 TAVR patients) showed a 1-year death or disabling stroke rate of 3.8% for TAVR vs. 8.4% for SAVR, significantly favoring TAVR (Blankenberg et al., 2024).
Symptomatic Intermediate-Risk Population
In the intermediate-risk population, three randomized studies reported outcomes for the composite endpoint of all-cause death or disabling stroke, with mixed findings across timepoints. The PARTNER 2 Cohort A trial (1,011 TAVR patients) reported 5-year event rates of 47.9% for TAVR and 43.4% for SAVR, showing no statistically significant difference between the two treatments (Makkar et al., 2020). A propensity score-matched analysis of the SAPIEN 3 cohort (783 TAVR patients) demonstrated a significant early benefit with TAVR (7.6% for TAVR versus 15.4% for SAVR at one year), though this advantage was not sustained over time and both groups showed substantially increased event rates of 40.2% for TAVR and 42.7% at five year that showed a neutral treatment effect (Madhavan et al., 2023). Similarly, the SURTAVI trial (864 TAVR patients) reported no difference between groups at five years, with rates of 31.3% for TAVR and 30.8% for SAVR (Van Mieghem et al., 2022).
Symptomatic Women (Across All Risk)
Among symptomatic women, the RHEIA trial reported a 1-year rate of 1.9% vs. 3.0% for SAVR, reflecting a neutral difference between interventions (Tchetche et al., 2025).
Comparisons of different valve types
Among the RCTs, two studies reported the composite endpoint of death or disabling stroke, comparing different transcatheter heart valve systems for TAVR, showing lower event rates after one or two years for MEVs as compared to SEV, but similar after five years and no clear superiority of SEV over a mixed group of valves.
Conclusion – Composite of all-cause mortality or disabling stroke
Across the included RCTs, the composite endpoint of all-cause mortality or disabling stroke was evaluated in 10 studies comparing TAVR with SAVR or CS, and in two studies comparing different transcatheter valve types. In the symptomatic low-risk population, early trial composite outcome findings showed a significant benefit for TAVR at one year that attenuated over time, becoming neutral, noninferior, or nonsignificant at two, four, five and seven years (Leon et al., 2021; Forrest et al., 2022; Mack et al., 2023; Leon et al., 2025). Meanwhile, NOTION-2 (Jørgensen et al., 2024) found no significant difference among low-risk patients aged ≤75 years at one year. One trial including symptomatic low- or intermediate-risk patients reported a benefit favoring TAVR at one year (Blankenberg et al., 2024), while findings were mixed for trials of intermediate-risk patients, showing some early advantages that were consistently not sustained at five years across studies (Makkar et al., 2020; Van Mieghem et al., 2022; Madhavan et al., 2023). Among symptomatic women, the RHEIA trial found no significant difference in 1-year outcomes between TAVR and SAVR (Tchetche et al., 2025).
Two studies evaluated valve type comparisons for this endpoint. The REPRISE III trial compared MEV (Lotus) with SEV (CoreValve/Evolut R) in high- and extreme-risk patients. MEV was associated with lower event rates at one and two years, but by five years, outcomes were similar, although MEV had fewer disabling strokes (Rizik et al., 2022). The PORTICO IDE trial reported comparable outcomes between the Portico SEV and the mixed group of commercially available valves at one and two years of follow-up. (Makkar et al., 2020b)
Taken together, evidence suggests that TAVR offers early clinical benefit in select low- and intermediate-risk populations, particularly within the first one to two years. However, long-term data demonstrate diminishing benefits, and in some cases, outcomes converge with those of SAVR. Comparisons between valve types reveal no definitive superiority, although individual valve designs may offer procedural or short-term clinical advantages in specific risk groups.
Composite of all-cause death or all stroke
Among the included studies that reported on the composite outcome of all-cause death or stroke, five compared TAVR with either SAVR or CS, and one compared different valve types. Across the five studies comparing TAVR with SAVR or CS, findings were inconsistent. In low-to-intermediate-risk patients, the DEDICATE-DZHK6 trial showed significantly better outcomes with TAVR at 1-year follow-up. In intermediate-risk populations, the SAPIEN 3 trial demonstrated early benefit at one year, favoring TAVR; however, longer-term data from both SAPIEN 3 and PARTNER 2 Cohort A showed comparable outcomes at five years. Among symptomatic women, both the RHEIA trial and a pooled analysis reported similar rates of death or stroke at one year between TAVR and SAVR, with no significant differences observed. In the single study comparing valve types (BEV vs. SEV), no statistically significant differences were reported in the composite outcome of all-cause death or stroke. No studies evaluated this composite outcome in exclusively low-risk patients. Detailed results are described in the sections below.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
Symptomatic Low- or Intermediate-Risk Population
One study in this risk category, the DEDICATE-DZHK6 trial, reported the composite of all-cause death or all stroke. Among 701 TAVR patients, the 1-year event rate for this composite was 5.4% in the TAVR group and 10.0% in the SAVR group, significantly favoring TAVR for non-inferiority (Blankenberg et al., 2024).
Symptomatic Intermediate-Risk Population
Two studies of intermediate-risk patients reported this composite. In the PARTNER 2 Cohort A trial, the 5-year rate of all-cause death or all stroke suggested comparable risk for the TAVR-treated patients, with 51.1% in the TAVR group versus 45.2% in the SAVR group (Makkar et al., 2020). Conversely, a propensity score-matched analysis of the SAPIEN 3 cohort from PARTNER 2 reported favorable results for TAVR at one year, with death or stroke occurring in 9.9% of TAVR patients and 17.4% of SAVR patients (Madhavan et al., 2023). However, by five years, this benefit had disappeared, with composite event rates of 44.8% in the TAVR group and 44.3% in the SAVR group (Madhavan et al., 2023).
Symptomatic Women (Across All Risk)
The RHEIA trial and the pooled analysis from RHEIA and PARTNER 3 both reported comparable outcomes between TAVR and SAVR. The RHEIA trial reported nearly identical 1-year outcomes: 4.2% in the TAVR group versus 4.4% in the SAVR group (Tchetche et al., 2025). The pooled analysis found 1-year rates of 3.5% for TAVR and 5.4% for SAVR, again reflecting a nonsignificant difference between groups (Eltchaninoff et al., 2025).
Comparisons of different valve types
Among the RCTs, one publication reported the composite of death or stroke comparing different transcatheter heart valve systems for TAVR, reporting no statistically significant difference between the two valve types (BEV or SEV) (GALILEO).
Conclusion – Composite of all-cause death or all stroke
No data are available for the composite of all-cause mortality or all stroke in symptomatic low-risk populations. In low- to intermediate-risk patients, TAVR was favored at one year in the DEDICATE-DZHK6 trial. In intermediate-risk patients, results were mixed: early benefit was seen in SAPIEN 3 at one year, but long-term data from both SAPIEN 3 and PARTNER 2 Cohort A showed comparable outcomes at five years. Among symptomatic women, both the RHEIA trial and pooled analysis showed similar rates of death or all stroke at one year between TAVR and SAVR. These findings suggest a possible early benefit of TAVR in selected intermediate and low-to-intermediate risk populations, but long-term outcomes for death or all stroke appear broadly similar between TAVR and SAVR. No statistically significant difference between the valve types SEV and BEV was noted for this composite outcome.
Randomized Controlled Trials – Asymptomatic AS
In contrast to the numerous RCTs for symptomatic patients with severe AS, there is a single, contemporary RCT on TAVR for asymptomatic patients –EARLY TAVR. EARLY TAVR randomized 901 patients with asymptomatic severe AS and preserved LVEF to prompt TAVR, or to close clinical monitoring at the outset. The primary outcome was a composite of death, stroke, or unplanned hospitalization for cardiovascular causes, at a median of 3.8 years. The authors reported that “a primary end-point event occurred in 122 patients (26.8%) in the TAVR group and in 202 patients (45.3%) in the clinical surveillance group” – a large, statistically-significant reduction in the primary outcome favoring early intervention. As a further breakdown: “Death occurred in 8.4% of the patients assigned to TAVR and in 9.2% of the patients assigned to clinical surveillance, stroke occurred in 4.2% and 6.7%, respectively, and unplanned hospitalization for cardiovascular causes occurred in 20.9% and 41.7%.” The authors concluded that “a strategy of early TAVR was superior to clinical surveillance in reducing the incidence of death, stroke, or unplanned hospitalization for cardiovascular causes” (Généreux 2025).
The EARLY TAVR trial data show that the positive trial result (favoring early, pre-emptive intervention) was driven by patients in the surveillance group who crossed over in the first six months (26%) because they became symptomatic or met other pre-specified criteria for progression of disease. The trial authors stated that “the percentage of patients who converted to aortic-valve replacement were 26.2% (116 patients) at 6 months, 47.2% (208 patients) at 1 year, and 71.4% (312 patients) at 2 years (Fig. S5, Kaplan-Meir estimates).” Over the 5-year trial duration, 87.0% of patients in the clinical surveillance group underwent aortic-valve replacement. There was no significant difference between groups in stroke and all-cause mortality over 5-year follow-up (accounting for the conversions to TAVR, in intention-to-treat analysis; Généreux 2025). The interpretation of this trial is controversial, however, as we discuss in depth in the CMS Coverage Analysis section.
Other trials on asymptomatic patients are underway or planned. The largest of the ongoing new trials is The Early Valve Replacement in Severe ASYmptomatic Aortic Stenosis Study (EASY-AS). This pragmatic, multicenter, prospective, parallel-group, open RCT is taking place in Europe (predominantly the UK), Australia and New Zealand. EASY-AS randomizes approximately 2,000 patients with severe asymptomatic AS to early AVR (SAVR or TAVR, as chosen by the local care team and patient) plus optimal medical therapy (OMT), or to “expectant management” (OMT alone with clinical surveillance). The primary outcome (recently amended) is a composite of cardiovascular death, stroke and heart-failure hospitalization (Richardson, et al., 2024).
Observational Studies – Symptomatic AS
All-cause mortality
The seven observational studies included in this review involved patients with AS treated with TAVR who participated in large registry-based or multicenter cohort studies. The studies evaluated mortality predictors and temporal trends after TAVR treatment, reporting mixed all-cause mortality outcomes that varied by symptom burden, time period, and procedural factors.
The OCEAN-TAVI registry, conducted across 14 centers in Japan, demonstrated an association between NYHA functional class and mortality among TAVR patients. Thirty-day mortality was 2.1% for NYHA class I, 1.2% for class II, 1.4% for class III, and 7.2% for class IV. At two years, the cumulative incidence of death rose with symptom severity, from 11.2% in class I to 30.0% in class IV, and adjusted regression models estimated over three times the risk of mortality at two years for class IV compared to class I patients (Taniguchi et al., 2022). The STS/ACC TVT Registry analysis from 793 sites in the US echoed these findings, showing that patients with preprocedural minimal or no symptoms (KCCQ-OS ≥ 75) had significantly lower 30-day mortality risk (1.0%) after TAVR than those with moderate-to-severe symptoms (1.8%), a finding that persisted for one year (Huded et al., 2023). In a separate temporal analysis of the TVT Registry, initially stable unadjusted 30-day mortality risk estimates (2.4% in 2019 vs. 2.2% in 2022) showed a significantly increased all-cause mortality trend over time when adjusted for patient characteristics and/or procedural factors. In-hospital mortality followed a similar trend, showing increased mortality when adjusted for patient characteristics and procedural factors (Arnold et al., 2024).
In contrast, the SWEDEHEART registry illustrated marked temporal improvements in TAVR outcomes. Thirty-day mortality for TAVR declined from 4.9% in 2013 to 1.6% in 2023, while patients in the SAVR group showed lower mortality that improved from 2.1% to 0.9% over this time period (Todt et al., 2026). One-year mortality in the TAVR cohort also declined (11.1% in 2013 to 6.9% in 2023). At five years, TAVR mortality dropped from 53.4% (2013) to 38.7% (2023), while SAVR mortality improved from 18.1% to 12.6%. A 10-year analysis revealed mortality rates of 83% for TAVR and 42% for SAVR, though only 0.5% of TAVR patients and 8% of SAVR patients remained at risk at 10 years due to censoring and loss to follow-up (Todt et al., 2026). The authors attributed the greater observed mortality risk for TAVR versus SAVR to the substantially increased volume of TAVR procedures for higher-risk patients compared to SAVR, reflecting the older age and higher comorbidity profile of patients undergoing TAVR, despite marked temporal reductions in mortality at each time point.
The OBSERVANT study, conducted at 93 centers in Italy, examined all-cause mortality among low and intermediate-risk patients undergoing TAVR or SAVR. The 1-year all-cause mortality was similar between groups (13.8% for TAVR vs. 13.6% for SAVR) (Barbanti et al., 2019). However, at five years, mortality was significantly higher with TAVR (44.5%) than with SAVR (35.8%) (Barbanti et al., 2019). In the RESPOND registry evaluating the Lotus valve, all-cause mortality was 2.6% at 30 days and 12.0% at one year (Van Mieghem et al., 2019). The Low Risk TAVR (LRT) trial, which used a historical control group, reported no 30-day deaths in the TAVR arm, compared with 1.7% in the SAVR group (Waksman et al., 2018).
These observational data showed highly variable results that highlight the diversity of study designs, patient populations, and settings, limiting the potential for synthesis of these findings. However, the studies suggested that symptom burden is a strong predictor of mortality, that outcomes have improved substantially over time, and that in some cohorts, TAVR mortality remains higher than SAVR in long-term follow-up, particularly in earlier cohorts or higher-risk groups.
CV mortality
In the RESPOND study, CV mortality was assessed in both the main and extension cohorts. In the main cohort, which included 1,014 patients in the ITT population and 996 patients in the as-treated population (those who received the Lotus valve), the 1-year CV mortality rate was 7.6% based on Kaplan–Meier estimates (74/996 events) (Van Mieghem et al., 2019). In contrast, the RESPOND extension cohort, which included 50 patients in the ITT population, reported zero CV deaths at 30 days (0 events) (Van Mieghem et al., 2019). These findings suggest relatively low CV mortality with the Lotus valve system at both early and intermediate-term follow-up.
Stroke
Across six observational studies and registries, the incidence of all strokes following TAVR or SAVR was evaluated, highlighting important trends across patient risk profiles, time periods, and valve technologies. In the STS/ACC TVT Registry, Huded et al. (2023) reported on a cohort of 231,285 TAVR patients. Among those with minimal symptoms (KCCQ-OS ≥ 75; n = 46,323), the 30-day stroke rate was 1.8%, while those with moderate-to-severe symptoms (KCCQ-OS < 75; n = 184,926) experienced a slightly higher rate of 2.2%; statistical significance of this difference between groups was not reported. Further analysis by Arnold et al. (2024) on 210,495 patients identified a temporal decline in unadjusted stroke and major vascular complications in TAVR patients, from 2.0% in Q1 2019 to 1.3% in Q1 2022 (p = NS), reflecting broader improvements in procedural safety over time. The SWEDEHEART registry, which captured outcomes from 21,383 patients treated between 2013 and 2023, mirrored this improvement trend. In-hospital stroke rates among TAVR recipients declined from 2.9% in 2013 to 1.9% in 2023, which approached statistical significance and was identical with the decline observed for SAVR patients over the same period (Todt et al., 2026).
In the OBSERVANT study, which examined a propensity score-matched cohort of 1,300 patients (650 TAVR and 650 SAVR), stroke incidence was comparable between groups. At 1-year follow-up, stroke occurred in 6.4% of TAVR patients versus 4.9% in SAVR patients (Barbanti et al., 2019). At five years, stroke rates increased to 13.2% for TAVR and 10.1% for SAVR. In this analysis, the differences in stroke outcomes for TAVR compared to SAVR patients were not statistically significant at either the short- or longer-term time points, and analyses reflected imprecise estimates and substantial uncertainty in the estimated comparative risk due to a low number of events (Barbanti et al., 2019).
In the RESPOND registry, which included 1,014 patients (of whom 996 received the Lotus valve), the 1-year stroke rate was 4.9% (Van Mieghem et al., 2019). A smaller extension cohort of 50 patients had a notably higher 30-day stroke rate of 6%, though the limited sample size may influence interpretation (Van Mieghem et al., 2019). The LRT trial, which compared 200 patients undergoing TAVR to 719 historical SAVR controls, reported a 30-day all-stroke rate of just 0.5% for TAVR, all of which were non-disabling (Waksman et al., 2018). Additionally, in-hospital stroke was observed in 0% of the TAVR group, compared to 0.6% in the SAVR control group (Waksman et al., 2018).
Collectively, these findings from observational and matched cohort studies suggest a general decline in stroke rates over time with TAVR, particularly in large-scale registries. However, comparative data from propensity-matched cohorts like OBSERVANT suggest that stroke incidence may still be modestly higher with TAVR than SAVR in the long term, warranting continued surveillance and patient selection considerations.
Disabling stroke
Based on data from large observational registries and feasibility studies, three prospective cohorts reported disabling stroke incidence following TAVR. In the RESPOND registry, which evaluated the Lotus valve system, the as-treated population (N = 996) experienced a disabling stroke rate of 1.7% at 30 days, with the cumulative incidence rising to 4.1% at one year (Van Mieghem et al., 2019). A separate RESPOND Extension cohort of 50 patients using a modified delivery system reported a 30-day disabling stroke rate of 2% (Van Mieghem et al., 2019). The OCEAN-TAVI registry, comprising 2,588 patients treated in Japan, provided in-hospital disabling stroke rates stratified by NYHA functional class: 2% in class I, 1% in class II, 1% in class III, and 4% in class IV. These differences were statistically significant, indicating increasing stroke risk with worsening functional status (Taniguchi et al., 2022). Additionally, the LRT trial, which compared 200 TAVR patients with 719 historical SAVR controls using inverse probability weighting, reported no cases of disabling stroke in the TAVR group during the 30-day follow-up period (Waksman et al., 2018). These findings suggest that, while disabling stroke rates are generally low across registries, patient baseline status, such as NYHA class, may influence risk profiles.
New permanent pacemaker implantation
Based on six observational studies included, the incidence of new permanent pacemaker implantation following TAVR versus SAVR demonstrated similar trends across propensity score-matched studies, national registries, and valve-specific cohorts. Evidence from these sources highlighted consistent differences in post-procedural conduction outcomes, particularly favoring SAVR in most comparisons.
Propensity Score-Matched and Observational Studies with Historic Controls
In the OBSERVANT study, which examined a propensity score-matched cohort of 1,300 patients (650 TAVR, 650 SAVR), the incidence of permanent pacemaker implantation was significantly higher in the TAVR group than in the SAVR group. At one year, 18.5% of TAVR patients required a pacemaker compared to just 7.3% in the SAVR group. This disparity persisted over time, with 5-year rates reaching 23.9% for TAVR and 10.2% for SAVR, indicating an elevated risk following TAVR (Barbanti et al., 2019). In contrast, in the LRT trial, which compared 200 TAVR patients with 719 historical SAVR controls, the 30-day pacemaker rate in TAVR patients was 6.5% overall, with similar in-hospital pacemaker implantation rates for TAVR (5.0%) and SAVR (4.5%) (Waksman et al., 2018).
National and Large-Scale Registries
In the STS/ACC TVT Registry (N = 210,495), pacemaker implantation rates following TAVR showed a declining trend, decreasing from 11.8% in early 2019 to 9.9% in early 2022 (Arnold et al., 2024). The SWEDEHEART registry, which followed 21,383 patients over a decade (2013–2023), reported a significant drop in in-hospital pacemaker implantation for TAVR patients, from 14.7% to 7.3%. In contrast, the SAVR population showed less variation over time, with rates shifting from 3.8% in 2017 to 4.3% in 2023 (Todt et al., 2026). Similarly, the OCEAN-TAVI registry (N = 2,588) observed stable in-hospital pacemaker implantation rates across NYHA functional classes, ranging from 7% to 8%, with no significant differences based on symptom severity (Taniguchi et al., 2022).
Prosthetic Valve Registries
The RESPOND registry, which focused on the mechanically expanded Lotus valve system, reported notably high pacemaker implantation rates in TAVR patients. At one year after the TAVR procedure, 32.3% of all patients and 37.2% of pacemaker-naive patients had received a device (Van Mieghem et al., 2019). In the RESPOND Extension cohort of 50 patients using a modified delivery system, the 30-day pacemaker implantation rate was reduced to 18% in the total population and 20% among those without a prior pacemaker (Van Mieghem et al., 2019).
Conclusion – New Permanent Pacemaker Implantation
Across observational studies, TAVR was consistently associated with a higher rate of permanent pacemaker implantation than SAVR. While recent registry data suggest a temporal decline in TAVR-associated conduction disturbances, the difference in pacemaker implantation rates between interventions remained statistically significant in several studies, particularly over long-term follow-up. These findings underscore the importance of procedural technique, valve selection, and patient-specific conduction risk assessment when considering TAVR.
Rehospitalization
Based on the three observational studies, large-scale registries, and matched cohorts reported the incidence of rehospitalization after TAVR, with a focus on heart failure (HF) and other cardiac-related events. In the OCEAN-TAVI registry involving 2,588 patients from Japan, the risk of HF-related rehospitalization at two years was significantly associated with baseline symptom severity. Analyses revealed that the risk of rehospitalization increased nonsignificantly for patients with NYHA class II compared to class I. However, rehospitalization risk was approximately three and four times greater for NYHA class III and IV patients compared to NYHA class I patients, respectively (Taniguchi et al., 2022). The OBSERVANT study, a propensity score-matched analysis of 1,300 patients (650 TAVR and 650 SAVR) in Italy, provided insights into cardiac and HF-specific rehospitalizations over a 5-year period. For general cardiac rehospitalizations, there was no significant difference between TAVR and SAVR at one year (21.9% vs. 23.6%) or at five years (48.2% vs. 43.0%). Regarding HF-specific rehospitalizations, both groups had similar 1-year rates (19.0% TAVR vs. 19.7% SAVR), but by five years, TAVR patients had a significantly more rehospitalizations (42.5% vs. 35.7%) (Barbanti et al., 2019). The RESPOND registry, which evaluated outcomes for 996 patients treated with the mechanically expanded Lotus valve system, focused on rehospitalization due to valve-related symptoms or congestive heart failure and reported a lower number of events. At one year, the cumulative incidence of such hospitalizations was 8.3% in the main cohort. In the smaller RESPOND Extension cohort of 50 patients, no hospitalizations for valve-related symptoms or CHF were reported within the 30-day follow-up period (Van Mieghem et al., 2019).
Together, these studies suggest that rehospitalization, particularly for heart failure, is influenced by baseline symptom severity, valve type, and patient selection. While TAVR patients with advanced symptoms reported higher risks, registry trends indicate relatively modest rates of valve-related rehospitalization in selected cohorts.
Bleeding
Based on five observational studies, bleeding outcomes were categorized as life-threatening, disabling, or major, and varied substantially by symptom severity, valve type, and procedural advancements over time. Data from national registries, device-specific cohorts, and matched observational studies provided details of bleeding risk following TAVR and SAVR.
In a large retrospective analysis from the STS/ACC TVT Registry involving 231,285 patients in the United States, 30-day rates of major or life-threatening/disabling bleeding were lower among patients with minimal or no symptoms (KCCQ-OS ≥ 75; 4.3%) compared to those with moderate-to-severe symptoms (KCCQ-OS < 75; 5.3%) (Huded et al., 2023). Temporal trends from the same registry demonstrated meaningful reductions in major bleeding complications from 5.6% in the first quarter of 2019 to 4.1% in the first quarter of 2022 (Arnold et al., 2024). In Sweden's SWEDEHEART registry, major in-hospital bleeding among TAVR patients dropped significantly from 7.8% in 2013 to 2.3% in 2023 (Todt et al., 2026). Conversely, SAVR patients saw a non-significant increase in in-hospital bleeding from 5.7% to 7.5% over the same period, reflecting improvements in transcatheter procedures but less change in surgical approaches (Todt et al., 2026). Similarly, the LRT trial compared 200 TAVR patients to 719 historical SAVR controls and showed more favorable bleeding complications for TAVR than SAVR patients. At 30 days, the combined rate of major vascular complications and life-threatening or major bleeding was 3.0% in the TAVR group (Waksman et al., 2018). For in-hospital bleeding specifically, VARC-2–defined life-threatening or major bleeding was significantly lower in the TAVR group (2.5%) than in the SAVR group (10.3%), with a between-group difference of -7.8% (Waksman et al., 2018).
The OCEAN-TAVI registry stratified in-hospital bleeding by baseline NYHA functional class in 2,588 Japanese patients. Life-threatening/disabling bleeding increased with symptom severity: 5% in NYHA I, 3% in NYHA II, 6% in NYHA III, and 11% in NYHA IV (Taniguchi et al., 2022). Major bleeding followed a similar trend, occurring in 9% of NYHA class I patients and 16% in class IV patients, although this difference did not reach statistical significance (Taniguchi et al., 2022). In the RESPOND registry, which evaluated the mechanically expanded Lotus valve in 996 as-treated patients, the 1-year cumulative incidence of life-threatening or disabling bleeding was 3.6% (Van Mieghem et al., 2019). Notably, in a smaller extension cohort of 50 patients using a revised delivery system, no life-threatening or disabling bleeding events were reported at 30 days (Van Mieghem et al., 2019), suggesting potential safety improvements with system modifications.
Overall, the observational data underscore a consistent trend of lower bleeding complications with improved TAVR techniques, reduced event rates over time, and variation by patient risk and symptom burden. Findings from newer valve systems and updated procedural strategies suggest continued improvements in bleeding safety profiles.
Patient-Reported Health Status Using KCCQ
The KCCQ was used in two publications from observational studies to assess post-procedural health status among patients undergoing TAVR. Both publications that reported this validated patient-reported outcome measure analyzed the STS/ACC TVT Registry. In a large-scale study involving 231,285 patients from the STS/ACC TVT Registry, Huded et al. (2023) stratified patients based on pre-procedural KCCQ Overall Summary (KCCQ-OS) scores into two distinct groups: those with minimal or no symptoms (KCCQ-OS ≥ 75; n = 46,323) and those with moderate-to-severe symptoms (KCCQ-OS < 75; n = 184,926). At 30 days post-TAVR, the minimally symptomatic group maintained significantly superior health status compared to the symptomatic group, with an adjusted mean difference in KCCQ-OS of 10.7 between groups. This health status advantage persisted through one year, with an adjusted mean score improvement of 9.1 for the minimally symptomatic patients compared to higher severity patients.
Beyond mean scores, patient-centric endpoints were also evaluated. The probability of being “alive and well” at one year, defined as survival with KCCQ-OS ≥ 60 and no decline of 10 or more points from baseline, was significantly higher among patients with minimal symptoms at baseline, indicating a durable benefit in quality-of-life post-procedure for this subgroup (Huded et al., 2023).
Composite Safety Outcome: death; stroke; stage 3 acute kidney injury/new dialysis; major, life-threatening, or disabling bleeding; and moderate or severe paravalvular regurgitation/leak
Observational analyses from the STS/ACC TVT Registry provided important insights into 30-day composite safety outcomes after TAVR, specifically a composite endpoint including death, stroke, stage 3 acute kidney injury or new dialysis, major or life-threatening/disabling bleeding, and moderate or severe paravalvular leak. In a retrospective cohort study of 231,285 patients, Huded et al. (2023) stratified outcomes by baseline symptom severity, using KCCQ-OS scores to divide patients into a minimally symptomatic group (KCCQ-OS ≥ 75; n = 46,323) and a moderately to severely symptomatic group (KCCQ-OS < 75; n = 184,926). The minimally symptomatic group had a significantly lower 30-day incidence of composite adverse events (8.1% vs. 9.9%) that remained statistically significant after adjusting for 37 baseline patient factors, suggesting that even among well-selected TAVR candidates, lower baseline symptom burden is associated with fewer early safety events.
Arnold et al. (2024) further evaluated temporal trends in a cohort of 210,495 TAVR patients from the same registry to assess safety outcomes from 2019 to early 2022. Over this 3-year span, the unadjusted 30-day composite event rate declined from 11.9% in early 2019 to 9.2% in early 2022 (p < 0.05), primarily driven by reductions in bleeding complications rather than changes in mortality or stroke. Year-over-year analysis revealed a significant decline in risk after adjusting for patient characteristics, that was attenuated after further accounting for procedural factors, suggesting that procedural improvements may already have been incorporated into care standards by 2019.
b. Differential Impact on Health Outcomes
The randomized trials and registry-based analyses included in this review employed various methods to determine whether the safety and effectiveness of TAVR vary by patient profile or procedural factors, such as subgroup interaction analyses, multivariable Cox regression, and propensity score matching. Across publications, TAVR relative to SAVR remained comparable across a wide range of patient characteristics and healthcare delivery factors.
Patient Characteristics
Age
Across publications, subgroup analyses evaluating the effect of age on outcomes following TAVR versus SAVR showed largely consistent results, suggesting no significant interaction between treatment effect and age in the short- to mid-term. In the DEDICATE-DZHK6 trial, TAVR was noninferior to SAVR for the composite of death or stroke at one year across both younger (<75 years) and older (≥75 years) patients, with approximately 50% reductions in composite outcome risk for TAVR compared to SAVR in both age groups (Blankenberg et al., 2024). The PARTNER 3 trial similarly found no evidence of heterogeneity by age group (<74 vs. ≥74 years) in the 2-year composite of death, stroke, or CV rehospitalization, suggesting similar benefits of TAVR across age groups (Leon et al., 2021). A post hoc subgroup analysis in the Evolut Low Risk Trial also supported this conclusion, with no significant interaction observed between age groups (<75 vs. ≥75 years) at two years (Forrest et al., 2022). Similarly, the NOTION trial reported no significant difference in 5-year all-cause mortality by age groups, reinforcing the consistency of treatment effect (Thyregod et al., 2019). However, in the 10-year follow-up of the NOTION trial, age ≥80 years at baseline emerged as a significant predictor of increased all-cause mortality, suggesting that age may not have short-term influence on comparative effectiveness, but does become a stronger determinant of mortality over the long term (Thyregod et al., 2024). Overall, these findings support the conclusion that age does not meaningfully modify the relative benefit of TAVR versus SAVR within the first five years, but advanced age may influence long-term mortality.
Sex
Subgroup analyses from multiple RCTs have examined whether sex modifies the comparative effectiveness of TAVR versus SAVR, with findings that are mixed across studies. In the DEDICATE-DZHK6 trial, results at one year suggested that TAVR may be more favorable in females than males for the composite outcome of death or stroke. Specifically, TAVR was associated with a statistically significant benefit in females and a similar benefit for males that was not statistically significant (Blankenberg et al., 2024). Similarly, in the CHOICE trial, female sex emerged as a significant multivariable predictor of lower 5-year mortality following TAVR, with women showing significantly better survival than men (Abdel-Wahab et al., 2020).
In contrast, several trials reported no significant interaction by sex. The PARTNER 3 trial found that the 1-year composite endpoint of death, stroke, or rehospitalization was similar between males and females (Leon et al., 2021). Similarly, in the Evolut Low Risk Trial, no significant interaction between treatment effect and sex was observed for the composite of all-cause mortality or disabling stroke at two years (Forrest et al., 2022). The NOTION trial also supported this consistency: a univariable subgroup analysis showed no heterogeneity in all-cause mortality by sex at five years (Thyregod et al., 2019), and sex was not a significant predictor of mortality in multivariate Cox regression analysis at the 10-year follow-up (Thyregod et al., 2024).
Body Mass Index
Subgroup analyses across several RCTs examined the influence of BMI on the comparative effectiveness of TAVR versus SAVR with mixed results. In the DEDICATE-DZHK6 trial, among low-to-intermediate risk patients, TAVR was noninferior to SAVR for the composite outcome of death or stroke at one year across BMI categories <25 and ≥30, though a statistically significant benefit favoring TAVR was observed in the BMI 25 to <30 subgroup (Blankenberg et al., 2024). In contrast, no significant interaction by BMI was observed in other trials, such as the Evolut Low Risk Trial at two years (BMI ≤30 vs. >30; p = 0.591) (Forrest et al., 2022) and the NOTION trial at five years (Thyregod et al., 2019). These findings suggest that BMI is unlikely to impact the relative benefits of TAVR vs. SAVR, although the results from DEDICATE-DZHK6 highlight a potential signal in the overweight subgroup that warrants further study.
STS-PROM Risk Scores
Subgroup analyses across several RCTs have examined whether STS-PROM surgical risk scores influence the comparative effectiveness of TAVR versus SAVR. The findings are largely consistent, with most studies showing no significant heterogeneity in treatment effects across surgical risk subgroups, although some exceptions indicate potential variation. In DEDICATE-DZHK6, TAVR was noninferior to SAVR for patients with STS-PROM ≤2% and >4% but significantly favored TAVR in the >2 to ≤4% group, though no interaction p-value was reported for the primary outcome of death or stroke at one year (Blankenberg et al., 2024). Similarly, the Evolut Low Risk Trial reported no significant interaction for the composite of all-cause mortality or disabling stroke at two years for STS score (<2 vs. ≥2; p = 0.444) (Forrest et al., 2022). In the PARTNER 3 trial, no heterogeneity of treatment effect was observed for patients with STS scores ≤1.8 vs. >1.8 for the primary endpoint of the composite of death from any cause, all stroke, or CV rehospitalization at two years (Leon et al., 2021). The NOTION trial also found no significant interaction for 5-year mortality based on a higher STS score threshold (<4 vs. ≥4) (Thyregod et al., 2019).
An exception was found in the CHOICE trial, where STS score was a significant multivariable predictor of 5-year mortality post-TAVR, indicating that higher surgical risk independently predicted worse outcomes (Abdel-Wahab et al., 2020). While DEDICATE-DZHK6 observed subgroup-specific differences in both BMI and STS risk strata, most trials did not report statistically significant interactions, suggesting consistent treatment effects across these variables. CHOICE adds complementary insight by showing that the STS score is an independent predictor of mortality, reinforcing the value of surgical risk assessment for absolute risk estimation, though not for comparative effectiveness between TAVR and SAVR.
Comorbidities, Symptom Status, and Functional Class
Across multiple RCTs, subgroup analyses consistently found no significant heterogeneity in treatment effect by comorbidities, symptom severity, or functional status for key composite outcomes.
In the Evolut Low Risk Trial, no significant interaction was observed at two years for the composite of all-cause mortality or disabling stroke across subgroups defined by NYHA functional class, baseline KCCQ score, chronic obstructive pulmonary disease (COPD), and baseline atrial fibrillation (Forrest et al., 2022). Similarly, the PARTNER 3 trial reported no heterogeneity of treatment effect for the primary composite endpoint (death, stroke, or CV rehospitalization at two years) by LVEF, NYHA class, atrial fibrillation, or KCCQ score (Leon et al., 2021). Consistent findings were also observed in the NOTION trial, with 5-year data showing no significant interaction for all-cause mortality across patients with or without peripheral vascular disease, diabetes mellitus, or stratified by LVEF (Thyregod et al., 2019). The extended 10-year follow-up confirmed that LVEF >50% was not significantly associated with all-cause mortality, and atrial fibrillation was not associated with the risk of stroke (Thyregod et al., 2024).
The DEDICATE-DZHK6 trial also explored a broad range of comorbidity and functional subgroups. For the primary endpoint of death or stroke at one year, TAVR was favored over SAVR in patients with NYHA class >II2, no coronary artery disease, no prior MI, no prior stroke, no cerebrovascular disease, no peripheral vascular disease, no COPD, and LVEF <55%, although interaction p-values were not reported (Blankenberg et al., 2024). In summary, while most trials report comparable TAVR benefit across various comorbidity and functional subgroups, DEDICATE-DZHK6 highlights potential areas of enhanced benefit in selected low-to-intermediate risk clinical profiles, which warrants further investigation.
Among the observational studies, two studies examined whether baseline symptom severity influenced outcomes (Huded et al., 2023; Taniguchi et al., 2022). A large retrospective analysis of the STS/ACC TVT Registry involving 231,285 patients found that patients with minimal or no symptoms (KCCQ-OS ≥ 75) had a lower risk of 1-year death compared to those with moderate-to-severe symptoms (Huded et al., 2023). However, this "minimally symptomatic" group showed smaller relative improvements in health status than symptomatic patients (Huded et al., 2023). Similarly, the OCEAN-TAVI registry reported that NYHA functional class was a significant predictor of mortality: while outcomes for NYHA classes I and II were similar, NYHA class IV was associated with markedly higher 2-year mortality compared to class I (Taniguchi et al., 2022).
Valve Morphology
In the NOTION-2 trial, an exploratory subgroup analysis was conducted to compare outcomes based on valve morphology (Jørgensen et al., 2024). Among patients with bicuspid valves, the 1-year composite risk of death or disabling stroke was not significantly different from that of patients with tricuspid valves. However, the incidence of moderate or greater paravalvular regurgitation was notably higher in the tricuspid TAVR group compared to the bicuspid surgical group, with an absolute risk difference of 9.1% (95% CI: 0.6% to 17.6%), indicating a three-fold increased risk in this subgroup (Jørgensen et al., 2024).
Healthcare Delivery and Procedural Factors
Access Site
Procedural access was a key determinant of comparative outcomes between TAVR and SAVR. In the PARTNER 2 Cohort A trial, the access site significantly influenced long-term results. Specifically, patients undergoing transthoracic TAVR experienced higher 5-year rates of death or disabling stroke compared to those treated with SAVR (59.3% vs. 48.3%), while outcomes for transfemoral TAVR were similar to SAVR (44.5% vs. 42.0%) (Makkar et al., 2020).
Findings from the Medtronic US High-Risk Pivotal Trial further underscored the importance of the access site, revealing a significant interaction between treatment modality and access route at one month. This led investigators to stratify all health status comparisons by iliofemoral versus non-iliofemoral access type (Arnold et al., 2021). At one month, patients receiving iliofemoral TAVR demonstrated significantly greater improvements in health status than those undergoing SAVR, with a treatment difference of 16.8 points in KCCQ-OS score. However, these differences diminished over time, with no meaningful differences in health status outcomes between iliofemoral TAVR and SAVR from six months through five years (Arnold et al., 2021). For non-iliofemoral patients, no significant differences in health status were observed between TAVR and SAVR at any follow-up point. However, due to the relatively small sample size in this subgroup, the confidence intervals for treatment differences were wide, limiting the precision of these findings (Arnold et al., 2021).
Temporal Trends and Real-World Evolution
Registry data reported a change in effectiveness over time. The SWEDEHEART registry (2013–2023) observed that in-hospital major adverse cardiac events for TAVR decreased from 6.5% to 3.3% over the decade (Todt et al., 2026). However, a US-based study of the STS/ACC TVT Registry found that, while unadjusted mortality remained stable between 2019 and 2022, the risk of 30-day mortality increased after adjusting for patient characteristics, suggesting that these findings warrant continued surveillance (Arnold et al., 2024).
Enrollment Phase (Learning Curve)
The PORTICO IDE trial analyzed safety outcomes by trial enrollment period and found a distinct difference (Makkar et al., 2020b). In the first half of enrollment, the Portico valve had significantly higher 30-day composite adverse events than commercial valves (16.0% vs. 7.7%), driven by major vascular complications (Makkar et al., 2020b). By the second half of the trial, this difference disappeared (11.6% vs. 11.5%), illustrating the impact of the procedural learning curve and technical refinements (Makkar et al., 2020b). The improved outcomes observed in the latter half of the trial may not reflect solely increased individual operator experience, but also the benefits of collective learning derived from cumulative use of the new device.
COVID-19 Impact:
Subgroup analyses in the DEDICATE-DZHK6 trial stratified by COVID-19 lockdown at admittance (Yes vs. No) and date of randomization (Before vs. After March 1, 2020) provided similar results, suggesting healthcare delivery shifts during the pandemic did not bias the primary outcome (Blankenberg et al., 2024).
Table 1. RCTs on TAVR for AS by the patient population
| Author year (Study name) |
Quality rating |
Tx; Comparator (N) |
Age, mean (SD) years |
Female (%) |
All-cause mortality (KM %) |
Stroke (KM %) |
MI (KM %) |
New permanent pacemaker implantation (KM %) |
Asymptomatic Severe AS Patients |
Merhi et al., 2022
(Evolut Low Risk) |
Fair |
TAVR: 76
SAVR: 62 |
75.0 (5.0);
73.3 (6.5) |
32; 21 |
30 days: 0.0, 3.2, p=0.15
1 year: 0.0, 4.8, p=0.05 |
30 days & 1 year (no change): 9.2, 3.2, p=0.15 |
Periprocedural: 0.0, 3.2, p=0.12 |
30 days: 24.0, 6.6, p<0.01
1 year: 24.0, 8.3, p=0.01 |
Généreux et al. 2025 (EARLY TAVR) |
Good |
TAVR: 455; Surveillance: 446 |
76 (6.0); 75.6 (6.0) |
28.8; 33.0 |
Median FU of 3.8 years: 8.4, 9.2; HR: 0.93 (95% CI: 0.60-1.44) |
Median FU of 3.8 years: 4.2, 6.7; HR: 0.62 (95% CI: 0.35-1.10) |
Periprocedural: 0.5, 0.5 |
Periprocedural: 5.7, 8.4 |
Symptomatic Severe AS at Low Risk |
Leon et al., 2021 (PARTNER 3 at 2 years) |
Fair |
TAVR: 496; SAVR: 454 |
73.3 (5.8); 73.6 (6.1) |
32.5; 28.9 |
1 year: 1.0, 2.5; HR: 0.41 (95% CI: 0.14-1.17)
2 years: 2.5, 3.2; HR: 0.75 (95% CI: 0.35-1.63) |
1 year: 1.2, 3.3; HR: 0.36 (95% CI: 0.14-0.92); 0.03
2 years: 2.5, 3.6; 0.66 (0.31-1.40); 0.28) |
1 year: 1.2, 2.2, p=0.23
2 years: 1.8, 2.7, p=0.36 |
1 year: 7.9, 5.8, p=0.18
2 years: 9.1, 7.0, p=0.21
Baseline pacemaker patients:
1 year: 7.7, 5.6, p=0.18
2 years: 8.9, 6.8, p=0.20 |
Mack et al., 2023 (PARTNER 3 at 5 years) |
Fair |
TAVR: 469; SAVR: 401 |
73.3 (5.8); 73.6 (6.1) |
32.5; 28.9 |
5 years: 10.0, 8.2; HR:
1.23 (95% CI: 0.79-1.90) |
5 years: 5.8, 6.4; 0.87
(95% CI 0.51-1.48) |
5 years: 2.1, 4.4; HR 0.48
(95% CI 0.22-1.05) |
5 years: 13.5, 10.4; HR 1.33
(95% CI 0.90-1.96)
(excluding baseline) |
Leon et al., 2025 (PARTNER 3 at 7 years) |
Fair |
TAVR: 496; SAVR: 454 |
73.3 (5.8); 73.6 (6.1) |
32.5; 28.9 |
7 years: 19.5, 16.8; HR: 1.17 (95% CI: 0.86-1.59) |
7 years: 8.5, 8.1; HR: 1.00 (95% CI 0.62-1.59) |
7 years: 6.0, 5.6; HR 0.99 (95% CI 0.56-1.75)* |
7 years: 17.3, 12.8; HR 1.38 (95% CI 0.97-1.97) |
Forrest et al., 2022 (Evolut Low Risk Trial at 2 years) |
Fair |
TAVR: 710; SAVR: 631 |
74.1 (5.8); 73.7 (5.9) |
36.4; 34.1 |
2 years: 3.5 (2.3-5.1), 4.4 (3.0-6.3); ?-0.9 (-3.0-1.2) |
2 years: 5.8 (4.3-7.9), 5.6 (4.0-7.7); ?0.2 (-2.3-2.8) |
2 years: 2.2 (1.3-3.6), 1.6 (0.9-3.0); ?0.6 (-0.9-2.1) |
2 years: 21.8 (18.9-25.2), 8.2 (6.2-10.8); ?13.6 (9.7-17.5)
Baseline pacemaker patients: 21.1 (18.2-24.4), 7.9 (6.0-10.4); ?13.2 (9.4-17.0) |
Forrest et al., 2023 (Evolut Low Risk Trial at 4 years) |
Fair |
TAVR: 691; SAVR: 610 |
74.1 (5.8); 73.7 (5.9) |
NR |
4 years: 9.0, 12.1, p=0.07) |
NR |
NR |
4 years: 24.6, 9.9, p<0.001* |
Sondergaard et al., 2019 (NOTION) |
Fair |
TAVR: 139; SAVR: 135 |
79.4 (4.9); 78.8 (4.6) |
47.5; 46.7 |
6 years: 42.5, 37.7, p=0.58 |
NR |
NR |
NR |
Thyregod et al., 2019 (NOTION) |
Fair |
TAVR: 145; SAVR: 135 |
Overall: 79.1 (4.8) |
NR |
5 years: 27.6, 28.9, p=0.75 |
5 years: 9.0, 7.4, p=0.65 |
5 years: 7.7, 7.4, p=0.96 |
5 years: 41.7, 7.8?, p<0.001* |
Thyregod et al., 2024 (NOTION) |
Fair |
TAVR: 145; SAVR: 135 |
79.2 (4.9); 79.0 (4.7) |
47.4; 46.2 |
10 years: 62.7, 64.0; HR 1.0 (95% CI: 0.7-1.3) |
10 years: 9.7, 16.4, p=0.1 |
10 years: 11.0, 8.2, p=0.4 |
10 years: 44.7, 14.0, p<0.01* |
Jørgensen et al., 2024 (NOTION 2) |
Fair |
TAVR: 187; SAVR: 183 (Tricuspid N=270; Bicuspid N=100) |
Tricuspid: 71.5; Bicuspid: 69.9 |
36.4; 38.3 |
1 year: 2.1, 1.1; HR 2.0 (95% CI 0.4-10.7) |
1 year: 5.4, 1.6; HR 3.3 (95% CI 0.9-12.0) |
1 year: 2.1, 1.6; HR: 1.3 (95% CI 0.3-5.9) |
1 year: 15.1, 8.0; HR 2.0 (95% CI 1.1-3.8) * |
Symptomatic Severe AS at Low or Intermediate Risk |
Blankenberg et al., 2024 (DEDICATE- DZHK6) |
Fair |
TAVI: 701 SAVR: 713 |
74.3 (4.6); 74.6 (4.2) |
44 |
1 year: 2.6, 6.2; HR 0.43 (95% CI 0.24-0.73) |
1 year: 2.9, 4.7; HR 0.61 (95% CI 0.35-1.06) |
1 year: 1.0, 2.1; HR 0.51 (95% CI 0.20-1.19) |
1 year: 11.8, 6.7; HR 1.81 (95% CI 1.27-2.61) |
Symptomatic Severe AS at Intermediate Risk |
Makkar et al., 2020 (PARTNER 2 at 5 years) |
Fair |
1,011; 1,021 |
81.5 (6.7); 81.7 (6.7) |
45.8; 45.2 |
2 years: 16.7, 18.0; HR 0.92 (95% CI 0.74-1.13)
5 years: 46.0, 42.1; HR 1.09 (95% CI 0.95-1.25) |
2 years: 9.5, 8.9; HR 1.04 (95% CI 0.78-1.40)
5 years: 15.3, 12.5; HR 1.15 (95% CI 0.89-1.49) |
2 years: 4.7, 4.3; HR 1.10 (95% CI 0.71-1.70)
5 years: 11.1, 8.2; HR 1.26 (95% CI 0.91-1.75) |
2 years: 11.8, 10.3; HR 1.17 (95% CI 0.89-1.53)
5 years: 15.5, 13.0; HR 1.20 (95% CI 0.94-1.54) |
Madhavan et al., 2023 (PARTNER 2 SAPIEN 3 & PARTNER 2 cohort A) |
Fair |
783; 783 (Propensity-matched cohort) |
81.7 (6.71); 81.5 (6.77) |
42.1; 42.8 |
1 year: 6.7, 12.2; HR 0.53 (95% CI 0.38-0.74)
5 years: 39.2, 41.4; HR 0.90 (95% CI 0.76-1.06) |
1 year: 4.5, 7.3; HR 0.62 (95% CI 0.40-0.94)
5 years: 13.4, 11.4; HR 1.09 (95% CI 0.80-1.48) |
NR |
1 year: 12.3, 8.9; OR 1.37 (95% CI 1.02-1.84)
5 years: 16.2, 11.7; OR 1.38 (95% CI 1.08-1.77) |
Van Mieghem et al., 2022 (SURTAVI) |
Fair |
TAVR: 864 SAVR: 796 |
79.9 (6.2); 79.7 (6.1) |
42.4; 45.0 |
2 years: 11.5, 10.5, p=0.53
5 years:30.0, 28.7, HR 1.06 (95% CI, 0.88-1.28) |
2 years: 6.0, 8.5; p=0.05
5 years: 11.6, 13.6; p=0.16) |
2 years: 2.7, 2.1; p=0.51
5 years: 6.2, 4.7; p=0.23 |
2 years: 30.9, 9.8; p <0.001
5 years: 35.8, 14.6; p <0.001 Excluding baseline:
2 years: 33.9, 10.0; p <0.001
5 years: 39.1, 15.1; p <0.001; HR 3.30 (95% CI, 2.61-4.17) |
Amrane et al., 2019 (SURTAVI Post hoc) |
Fair |
TAVR: 864 SAVR: 796 |
79.9 (6.2); 79.7 (6.1) |
42.4; 45.0 |
% of patients, TAVR, SAVR:
0-30 days: 18 (2.1), 13 (1.6), p=0.50
31-120 days: 10 (1.2), 16 (2.1), p=0.16
121-365 days: 28 (3.4), 23 (3.1), p=0.76 |
% of patients, dead, alive¥
0 to 30 days: TAVR: 67.2, 2.7, p<0.05; SAVR: 19.2, 5.3, p=NS< 0.05
31 to 120 days: TAVR: 14.3, 3.1, p=NS; SAVR: 66.1, 5.6, p<0.05
121 to 365 days: TAVR: 9.2, 4.6, p=NS; SAVR: 23.9, 5.5), p<0.05 |
% of patients, dead, alive¥
0-30 days: TAVR: 25.3, 0.5, p<0.05 SAVR: 15.4, 0.6, p<0.05
31-120 days:
TAVR: 10.0, 0.7, p<0.05 SAVR: 12.5, 0.8, p<0.05
121-365 days: TAVR: 8.4, 1.3, p<0.05 SAVR: 0.0, 0.9, p=NS |
% of patients, dead, alive ¥
0 to 30 days:
TAVR: NR 14.9, 25.8, p=NS; SAVR: 14.3, 6.4, p=NS
31 to 120 days: TAVR: 10.0, 27.1, p=NS; SAVR: 12.5, 6.9, p=NS
121 to 365 days: TAVR: 28.6, 28.8, p=NS; SAVR: 8.7, 8.4, p=NS |
Symptomatic Severe AS at Intermediate-High Risk |
Thiele et al., 2020 (SOLVE TAVI) |
Good |
SEV: 218 BEV: 215 |
81.7 (5.3); 81.5 (5.7) |
52.1; 50.2 |
SEV: 3.2, BEV: 2.3; ?-0.94 (90% CI: -4.79-2.91); Pequivalence<0.001 |
SEV: 0.5, BEV: 4.7; ?4.20 (90% CI: 0.11-8.28); Pequivalence=0.003 |
NR |
SEV: 23.0, BEV: 19.2; ?-3.85 (90% CI: -10.41-2.72); Pequivalence=0.06 |
Feistritzer et al., 2025 (SOLVE TAVI) |
Fair |
SEV: 218 BEV: 215 |
81.7 (5.3); 81.5 (5.7) |
52.1; 50.2 |
SEV: 48.5, BEV: 47.6; HR: 0.98 (95% CI: 0.74-1.29) |
SEV: 2.2, BEV: 9.6; HR: 4.84 (95% CI: 1.65-14.18) |
SEV: 0, BEV: 2.5 p=0.02 |
SEV: 24.9, BEV: 22.8; HR: 0.75 (95% CI: 0.52-1.08) |
Symptomatic Severe AS at High Risk |
Arnold et al., 2021 (Medtronic Core Valve US High-Risk Pivotal Trial) |
Fair |
TAVR: 377 SAVR: 336 |
83.2 (7.1); 83.5 (6.3) |
47.2; 47.0 |
NR |
NR |
NR |
NR |
Feldman et al., 2018 (REPRISE III) |
Good |
MEV: 520 SEV: 262 |
82.8 (7.1); 82.9 (7.6) |
50.1; 52.1 |
TTE rates %, MEV, SEV:
30-day: 2.5, 2.3; ?0.2 (95% CI: -1.9-2.3)
1 year: 11.9, 13.5; ?-1.5 (95% CI: -6.2-3.1) |
TTE rates %, MEV, SEV:
30-day: 4.8, 4.3; ?0.5 (95% CI: -2.3-3.4)
1 year: 7.0, 9.4; ?-2.4 (95% CI: -6.4-1.5) |
TTE rates %, MEV, SEV:
30-day: 0.7, 1.3; ?-0.7 (95% CI: -2.1-0.8)
1 year: 3.2, 4.4; ?-1.1 (95% CI: -3.9-1.6) |
Pacemaker-naïve patients: TTE rates %, MEV, SEV:
30-day: 35.5, 19.6; ?15.9 (95% CI: 9.4-22.4)
1 year: 41.4, 23.0; ?18.4 (95% CI: 11.5-25.3) |
Reardon et al., 2019b (REPRISE III) |
Good |
MEV: 136 SEV: 137 |
Overall: 82.8 (7.3) |
Overall: 51.0 |
TTE rates %, MEV, SEV: 21.3, 22.5; HR: 0.94 (95% CI: 0.69-1.26) |
TTE rates %, SEV, MEV: 11.4, 8.4; HR: 0.75 (95% CI: 0.48-1.17) |
TTE rates %, SEV, MEV: 6.3, 6.1; HR: 0.93 (95% CI: 0.52-1.68) |
TTE rates %, pacemaker-naïve patients, SEV, MEV: 26.1, 41.7; HR: 1.87 (95% CI: 1.41-2.49) |
Rizik et al., 2022 (REPRISE III) |
Good |
MEV: 607 SEV: 305 |
Overall: 82.8 (7.3) |
Overall: 50.8 |
TTE rates %: MEV, SEV: 50.9, 52.8; HR: 0.95 (95% CI: 0.78-1.16) |
TTE rates %: MEV, SEV: 14.1, 15.3; HR: 0.84 (95% CI: 0.57-1.24) |
TTE rates %: MEV, SEV: 11.0, 12.4; HR: 0.90 (95% CI: 0.56-1.44) |
TTE rates %: MEV, SEV, pacemaker-naive patients: 48.6, 35.2; HR: 1.67 (95% CI: 1.28-2.18) |
Abdel-Wahab et al., 2020 (CHOICE) |
Good |
BEV: 121 SEV: 120 |
81.9 (6.7); 79.6 (15.8) |
57.0; 71.7 |
53.4 (44.5-62.9), 47.6 (38.6-57.4) |
17.5, 16.5, p=0.73 |
1.6, 6.1, p=0.08 |
25.4, 40.4, p=0.01 |
Makkar et al., 2020b (PORTICO IDE) |
Good |
Portico valve (PV): 381 Commercially available valve (CAV): 369 |
83.0 (7.6); 83.7 (7.0) |
52.0; 53.4 |
Difference (95% CI); PV vs CAV:
30 days: 3.5, 1.9; 1.5 (-0.8-3.9)
1 year: 14.3, 12.0; 2.4 (-2.6-7.3)
2 years: 22.3, 20.2; 2.1 (-4.0-8.1) |
NR |
NR |
30-day: PV: 27.7, CAV: 11.6; ?16.1 (95% CI: 10.0-22.2) |
Symptomatic Severe AS at All Risk categories |
Herrmann et al., 2024 (SMART) |
Good |
SEV: 355; BEV: 361 |
80.1 (6.3); 80.3 (6.1) |
87.9; 85.6 |
1 year: 5.1, 5.9; -0.7 (90% CI: -3.5-2.1) |
NR |
NR |
30 days: 12.1, 7.8, HR: 1.61 (95% CI: 0.98-2.65) |
Tchétché et al., 2024 (SMART) |
Fair |
SEV: 312; BEV: 309 |
80.2 (6.3); 80.1 (6.0) |
100 |
1 year: 5.2, 6.2; HR: 0.84 (95% CI: 0.43-1.63) |
NR |
NR |
30 days: 11.8, 7.6, p=0.07 |
Tchetche et al., 2025 (RHEIA) |
Fair |
TAVR: 215 SAVR: 205 |
73.1 (4.5); 73.3 (5.2) |
100 |
30 days: 0.5, 0.5; ?: 0.0 (95% CI: -1.3-1.3)
1 year: 0.9, 2.0; ?: -1.0 (95% CI: -3.3-1.3); HR=0.47 (95% CI: 0.09-2.59) |
30 days: 1.9, 1.0; ?0.9 (95% CI: -1.4-3.2)
1 year: 3.3, 3.0; ?0.3 (95% CI: -3.0-3.7); HR: 1.12 (95% CI: 0.37-3.32) |
30 days: 0.0, 0.5; ?: -0.5 (95% CI: -1.4-0.5)
1 year: 0.0, 1.0; ?: -1.0 (95% CI: -2.3-0.4) |
30 days: 7.9, 2.9; ?5.0 (95% CI: 0.7-9.3)
1 year: 8.8, 2.9; ?5.9 (95% CI: 1.5-10.4) |
Eltchaninoff et al., 2025 (RHEIA and PARTNER 2) |
Fair |
TAVR: 376 SAVR: 336 |
73.4 (4.78); 73.3 (5.18) |
100; 100 |
1 year: 1.1, 2.1; ?: -1.0 (95% CI: -2.9-0.8) |
1 year: 2.7, 3.9; ?: -1.2 (95% CI: -3.9-1.4) |
30 days: 0.3, 1.5; ?: -1.2 (95% CI: -2.6-0.2) |
1 year: 6.8, 5.0; ?1.8 (95% CI: -1.7-5.3) |
Okuno et al., 2022 (GALILEO) |
Fair/Poor |
SEV: 499 BEV: 757 |
81.0 (6.6); 80.2 (6.8) |
59.3; 39.0 |
2 years: 11.4, 9.3; adjHR: 1.26 (95% CI: 0.78-2.05) |
2 years: 5.1, 3.7; adjHR: 0.86 (95% CI: 0.43-1.73) |
2 years: 3.2, 3.1; adjHR: 1.45 (95% CI: 0.68-3.10) |
NR |
Abbreviations: ANCOVA: Analysis of covariance; AS: Aortic stenosis; BEV: Balloon-expandable valve; CI: Confidence interval; CS: Clinical surveillance; FU: Follow-up; HR: Hazard ratio; KCCQ: Kansas City Cardiomyopathy Questionnaire; KCCQ-OS: Kansas City Cardiomyopathy Questionnaire Overall Summary score; KM: Kaplan–Meier; MEV: Mechanically expanded valve; MI: Myocardial infarction; NR: Not reported; OS: Overall Summary; PV: Portico valve; SAVR: Surgical aortic valve replacement; SD: Standard deviation; SE: Standard error; SEV: Self-expanding valve; TAVR: Transcatheter aortic valve replacement; TTE: Time-to-event
*Patients with a pre-existing permanent pacemaker or defibrillator were excluded from the analysis.
? There was discrepancy in the publication hence data reported from the table in the results section and not from the abstract
¥ p-value based on log-rank for dead vs alive
Note: The reported sample size reflects the number of patients who completed the specified follow-up period, as derived from trials with multiple publications reporting outcomes at different follow-up durations.
Table 2: Summary table of RCTs reviewed to assess TAVR vs SAVR/CS
| Outcome |
Reviewed Studies (Study Quality) |
Findings |
Quality of Body of Evidence |
All-cause mortality |
16 studies (28 publications: 8 good, 19 fair, 1 poor) *
- 6,039 patients treated with TAVR among the 18 publications (10 studies) that compared with SAVR/CS
- 4,270 patients treated with TAVR among the 10 publications (6 studies) that compared different valve platforms
|
- Across the 7 studies, TAVR and SAVR/CS had comparable all-cause mortality, with no statistically significant differences. However, two trials reported a 1-year mortality benefit for TAVR over SAVR: one examined asymptomatic patients (Evolut Low Risk) and the other the low-to-intermediate-risk population (DEDICATE-DZHK6). One trial (PARTNER 2 SAPIEN 3) reported that at 1 year, TAVR was significantly better than SAVR, but at 5-year mortality rates were similar.
- Across 6 studies, no statistically significant differences in all-cause mortality were observed among the valve platforms studied (e.g., BEV, SEV, MEV).
|
High |
Cardiovascular Mortality |
13 studies (20 publications: 5 good, 14 fair, 1 poor)
- 5,565 patients treated with TAVR among the 15 publications (10 studies) that compared with SAVR/CS
- 2,371 patients treated with TAVR among the 5 publications (3 studies) that compared valve types
|
- Across the 8 studies, TAVR and SAVR/CS showed comparable cardiovascular mortality, with no statistically significant differences reported. However, one trial reported a 1-year cardiovascular mortality benefit for TAVR over SAVR among the low-to-intermediate-risk population (DEDICATE-DZHK6). One trial (PARTNER 2 SAPIEN 3) reported that at 1 year, TAVR was significantly better than SAVR, but at 5-year cardiovascular mortality rates were similar.
- Across 3 studies, no statistically significant differences in cardiovascular mortality were observed among the valve platforms studied (e.g., BEV, SEV, MEV).
|
High |
Stroke |
16 studies (23 publications: 6 good, 16 fair, 1 poor)
- 6,039 patients treated with TAVR among the 16 publications (12 studies) that compared with SAVR/CS
- 2804 patients treated with TAVR among the 7 publications (4 studies) that compared valve types
|
- Across 8 studies, TAVR and SAVR/CS showed a comparable rate of stroke, with no statistically significant differences reported. However, three studies examining patients from low- to intermediate-risk populations (PARTNER 3, PARTNER 2 SAPIEN 3, and the SURTAVI trial) reported a statistically significant reduction in stroke with TAVR compared to SAVR at early follow-up of 1-2 years, but at 5 years, stroke rates were similar. One study reported an increase in stroke in the TAVR group at 1 year (NOTION 2).
- Across 3 studies, no statistically significant differences in stroke were observed among the valve platforms studied (e.g., BEV, SEV, MEV). However, one study (SOLVE TAVI) reported a statistically lower stroke rate with SEV at both 30 days and 5 years, favoring SEV over BEV.
|
Moderate |
Disabling Stroke |
14 studies (21 publications: 6 good, 15 fair)
- 5,643 patients treated with TAVR among the 15 publications (11 studies) that compared with SAVR/CS
- 1,610 patients treated with TAVR among the 6 publications (3 studies) that compared valve types
|
- Across the 9 studies, TAVR and SAVR/CS showed comparable disabling stroke, with no statistically significant differences reported. Whereas 2 studies (DEDICATE-DZHK6 and PARTNER 2 SAPIEN 3) reported statistically significant reduction in disabling stroke with TAVR compared to SAVR at 1- and 5-year FU.
- Across 2 studies, no statistically significant differences in disabling stroke were observed among the valve platforms studied (e.g., BEV, SEV). However, one trial (REPRISE III) reported a statistically lower disabling stroke rate with MEV at 1, 2, and 5 years FU, favoring MEV over SEV.
|
Moderate |
New permanent pacemaker implantation |
17 studies (25 publications: 8 good, 17 fair)
- 6,039 patients treated with TAVR among the 16 publications (12 studies) that compared with SAVR/CS
- 3,014 patients treated with TAVR among the 9 publications (5 studies) that compared valve types
|
- Across the 12 studies, 4 showed comparable pacemaker implantation rate among TAVR and SAVR/CS with no statistically significant differences reported. However, 8 studies reported that the rate of new pacemaker implantation (excluding pacemakers or ICDs at baseline) was statistically significantly higher with TAVR than with SAVR at FU, ranging from 1 to 10 years.
- Across 5 studies: One (REPRISE III) trial reported a statistically higher rate of pacemaker implantation with MEV at 1, 2, and 5 years FU, favoring MEV over SEV. One trial (CHOICE) reported a statistically higher rate of pacemaker implantation with SEV than BEV at 1 year FU, and two trials reported a higher rate of pacemaker implantation with SEV than BEV from 30 days to 5 years FU, but did not reach statistical significance. One trial (PORTICO IDE) reported that the 30-day pacemaker implantation rate was significantly higher with the PV than with the CAV group.
|
High |
Myocardial infarction |
15 studies (21 publications: 5 good, 15 fair, 1 poor)
- 5,041 patients treated with TAVR among the 15 publications (11 studies) that compared with SAVR/CS
- 2804 patients treated with TAVR among the 6 publications (4 studies) that compared valve types
|
- Across the 11 studies, TAVR and SAVR/CS showed a comparable rate of MI, with no statistically significant differences reported.
- Across 4 studies, no statistically significant differences in MI were observed among the valve platforms studied (e.g., BEV, SEV, MEV), except one trial that reported a significantly lower MI incidence with SEV compared to BEV at 5 years (SOLVE TAVI).
|
High |
Reintervention |
11 studies (20 publications: 4 good, 16 fair)
- 4,993 patients treated with TAVR among the 15 publications (9 studies) that compared with SAVR/CS
- 1,590 patients treated with TAVR among the 5 publications (2 studies) that compared valve types
|
- Across the 9 studies, 7 studies reported that TAVR and SAVR/CS showed a comparable rate of reintervention, with no statistically significant differences reported. However, two studies in intermediate-risk populations (PARTNER 2 and SURTAVI) reported significantly higher reintervention rates with TAVR at 5 years.
- In 1 study, no statistically significant differences in the rate of reintervention were observed among the valve platforms studied (BEV vs SEV). However, one (REPRISE III) trial reported a statistically higher reintervention rate with SEV at 1 and 2 years FU, favoring SEV over MEV, but at 5 years the groups were comparable.
|
High |
PRO: Kansas City Cardiomyopathy Questionnaire |
13 studies (16 publications: 4 good, 12 fair)
- 4,687 patients treated with TAVR among the 12 publications (10 studies) that compared with SAVR/CS
- 2,340 patients treated with TAVR among the 4 publications (3 studies) that compared valve types
|
- Across the 10 studies, TAVR and SAVR/CS showed greater improvement in health status with TAVR at early time points, particularly within the first month after the procedure. Long-term patient-reported outcomes are largely comparable to those achieved with surgery, with no statistically significant differences reported.
- Across 3 studies, in 2 studies, no statistically significant differences in health status were observed among the valve platforms studied (e.g., BEV, SEV, MEV). However, one (SMART) trial found that SEV was associated with significantly greater improvements in KCCQ at 1 year than BEV.
|
Moderate |
Composite of all-cause death, all stroke (disabling or non-disabling), or cardiovascular rehospitalization |
8 studies (10 publications: 1 good, 9 fair)
- 3,308 patients treated with TAVR among the 10 publications (8 studies) that compared with SAVR/CS
- No patients treated with TAVR among the 0 publications (0 study) that compared valve types
|
- Across the 8 studies, findings were inconsistent.
In four studies, in asymptomatic, low-risk, and female populations, TAVR was favored over SAVR (EARLY, Evolut Low Risk Trial, RHEIA, Pooled RHEIA, and PARTNER 3). In 2 studies (PARTNER 3, SAPIEN 3), TAVR was associated with benefits, but these benefits attenuated over longer-term follow-up. In one study outcome was comparable (NOTION 2). However, in one study, the results favored SAVR over TAVR (PARTNER 2 Cohort A).
| NA |
Composite of all-cause mortality or disabling stroke |
12 studies (17 publications: 5 good, 12 fair)
- 5,518 patients treated with TAVR among the 13 publications (10 studies) that compared with SAVR/CS
- 1,624 patients treated with TAVR among the 4 publications (2 studies) that compared valve types
|
- Across the 10 studies, findings were inconsistent. In low-risk patients, results were mixed: early benefits were observed in PARTNER 3 at 1 year, but long-term outcomes were comparable at 7 years. The Evolut Low Risk Trial TAVR was comparable to SAVR at 2 years but favored TAVR at 4 years. In one study in low- to intermediate-risk patients, TAVR was favored at 1 year (DEDICATE-DZHK6). In intermediate-risk patients, results were mixed: early benefit was observed with SAPIEN 3 at 1 year, but long-term outcomes were comparable at 5 years. The other 6 studies showed comparable outcomes between TAVR and SAVR, with no statistically significant differences.
- Across 2 studies, no statistically significant differences in composite outcome were observed among the Portico SEV and the mixed group of commercially available valves at 1 and 2 years (PORTICO IDE). However, MEV was associated with lower event rates at 1 and 2 years, but by 5 years, outcomes were similar (REPRISE III).
|
NA |
Composite of all-cause death or stroke |
6 studies (6 publications: 5 good, 1 poor)
- 2,786 patients treated with TAVR among the 5 publications (5 studies) that compared with SAVR/CS
- 1,256 patients treated with TAVR among the 1 publication (1 study) that compared valve types
|
- Across the 5 studies, findings were inconsistent. In one study in low- to intermediate-risk patients, TAVR was favored at 1 year (DEDICATE-DZHK6). In intermediate-risk patients, results were mixed: early benefit was seen in SAPIEN 3 at 1 year, but long-term data from both SAPIEN 3 and PARTNER 2 Cohort A showed comparable outcomes at 5 years. Among symptomatic women, both the RHEIA trial and pooled analysis showed similar rates of death or stroke at 1 year between TAVR and SAVR.
- In the included study, no statistically significant differences in the composite of all-cause death or stroke were observed among the valve platforms studied (BEV vs SEV).
|
NA |
*Only publications reporting on all-cause mortality are included. The Publication reporting on survival is not included.
Note: Findings are presented at the study level rather than the publication level to enhance clarity and facilitate interpretation.
3. Quality of Evidence from Primary Studies
Overall, the certainty of evidence from RCTs was high for all-cause mortality, supported by numerous trials with adequate randomization, low risk of bias, and precise estimates despite some indirectness and moderate inconsistency. Most trials demonstrated consistently nonsignificant differences in all-cause mortality between groups, with a small number of trials favoring TAVR treatment. For stroke, the overall certainty was moderate, reflecting generally good study designs that were tempered by moderate imprecision and inconsistency due to mixed findings across trials. Evidence for MI was rated high, as results were consistent across studies, confidence intervals were narrow, and no meaningful inconsistency was observed. The certainty of evidence for new permanent pacemaker implantation was also high, given consistent direction and magnitude of effect across trials, precise estimates, and minimal concern for publication bias. For reintervention, overall certainty was high, supported by adequate power and precision, at least for the duration of the studies. In contrast, evidence for health status measured by KCCQ was rated moderate, reflecting heterogeneity in results across trials and moderate imprecision, with benefits favoring TAVR primarily at early follow-up that subsequently attenuated over time.
In turn, the large observational studies were generally rated fair quality in the USPSTF assessment (see Table 4 in Appendix B) due to their nonrandomized design, but were recognized for strong external validity, large sample sizes, and real-world applicability, including the STS/ACC TVT Registry, SWEDEHEART registry, and OCEAN-TAVI registry.
Please see Appendix B for tables and further discussion.
4. Applicability to the Medicare Population
Overall, while the age and sex profiles of study populations align well with those of Medicare beneficiaries, and observational studies improve representativeness, the restrictive exclusion criteria of RCTs limit their full applicability to the broader, more medically complex Medicare population. Consequently, extrapolation of RCT findings to typical Medicare beneficiaries should account for underrepresentation of patients with advanced comorbidities, frailty, complex coronary disease, and alternative access needs. The large observational registries included patients with severe renal disease, chronic lung disease, frailty, and other high-risk characteristics, supporting greater external validity for real-world application, albeit with the inherent limitations of non-randomized designs.
Age: Across RCTs, the age profile of enrolled patients was well-aligned with the Medicare population. Most RCTs enrolled older adults, with mean/median ages ranging from 73.1 years (Tchetche et al., 2025) to 83.2 years (Arnold et al., 2021; Makkar et al., 2020b), reflecting the population most affected by severe AS and most relevant to Medicare beneficiaries. Observational studies, particularly large registry-based analyses, further strengthened applicability by including even older patients, mostly with broader comorbidity profiles, which are representative of real-world Medicare populations.
Sex: Regarding sex representation, both RCTs and observational studies included meaningful proportions of women, ranging from approximately 28.5% (Généreux et al., 2025) to 59.3% (Okuno et al., 2022). This participation is consistent with the sex distribution of AS in older adults and is broadly representative of the Medicare population. While some trials, such as Evolut Low Risk, enrolled fewer women than men (women 21%), this imbalance is unlikely to substantially limit the applicability of findings by sex.
Race/Ethnicity: In contrast, representation of race and ethnicity was more limited, with only four studies providing specific data. Across those RCTs, participants were predominantly White, with relatively low enrollment of racial and ethnic minority groups. Observational studies showed modestly improved inclusion of non-White patients compared with RCTs, reflecting the use of national registries and real-world data sources; however, minority representation is below the proportions observed in the overall Medicare population. In several studies, race and ethnicity data were incomplete or inconsistently reported, further limiting assessment of differential outcomes across groups.
Clinical eligibility criteria: The analysis of study populations across the included sources indicates that, while large observational registries generally enrolled broad and clinically diverse patient populations, RCTs applied restrictive eligibility criteria that excluded comorbidities common among older adults, thereby creating a potential gap between trial populations and patients treated in routine clinical practice. The primary RCTs employed extensive exclusion criteria. Notably, bicuspid aortic valves, despite being a frequent etiology of AS, were explicitly excluded from several major trials, including the Evolut Low Risk Trial (Forrest et al., 2022), PARTNER 3 (Leon et al., 2021), SURTAVI (Van Mieghem et al., 2022), DEDICATE-DZHK6 (Blankenberg et al., 2024), and the Low Risk TAVR trial (Waksman et al., 2018). Similarly, severe renal insufficiency, including end-stage renal disease requiring dialysis, was a common exclusion across RCTs. EARLY TAVR (Généreux et al., 2025) and RHEIA (Tchetche et al., 2025) excluded patients with estimated glomerular filtration rate (eGFR) <30 ml/min, while PARTNER 2 cohort A (Makkar et al., 2020) and SURTAVI (Van Mieghem et al., 2022) excluded patients with serum creatinine >3.0 mg/dL or creatinine clearance <20 cc/min. These exclusions contrast with real-world populations in which advanced kidney disease is relatively common among older adults undergoing TAVR evaluation. Severe lung disease was also frequently excluded. Conditions such as severe chronic obstructive pulmonary disease (COPD), defined by FEV1 <50% or <750 cc, or dependence on home oxygen, were exclusionary in EARLY TAVR (Généreux et al., 2025), NOTION (Thyregod et al., 2024), and SURTAVI (Van Mieghem et al., 2022). In addition, frailty and cognitive impairment were commonly used exclusion criteria. Significant frailty was excluded in both the LRT trial (Waksman et al., 2018) and EARLY TAVR (Généreux et al., 2025), while severe dementia was an exclusion in REPRISE III (Feldman et al., 2018) and SURTAVI (Amrane et al., 2019). As a result, RCT populations included healthier, more functionally robust patients than those typically encountered in routine clinical care. In contrast, large-scale observational registries included patients with these comorbidities and more closely resembled real-world practice. The STS/ACC TVT Registry (Huded et al., 2023) and SWEDEHEART (Todt et al., 2026) enrolled patients with advanced comorbid conditions, including those on chronic dialysis (approximately 1.7–3.0%) and those with severe lung disease (up to 8.2%), supporting broader applicability to older and comorbid populations.
Beyond comorbidities, RCTs also commonly restricted disease-specific clinical history and concomitant treatments to ensure more homogeneous cohorts. Many trials excluded patients with complex coronary artery disease (CAD), defined either by a SYNTAX score >22 or >32, or by the presence of untreated, clinically significant CAD requiring revascularization, as seen in SURTAVI (Van Mieghem et al., 2022), RHEIA (Tchetche et al., 2025), and SMART (Herrmann et al., 2024). In contrast, registry data indicate that CAD is highly prevalent in clinical practice, affecting up to 71.5% of patients undergoing TAVR. Similarly, severe concomitant valvular disease, including grade 3+ or 4+ mitral or tricuspid regurgitation, was frequently excluded in RCTs such as REPRISE III (Feldman et al., 2018) and EARLY TAVR (Généreux et al., 2025). However, observational data from the OCEAN-TAVI registry (Taniguchi et al., 2022) demonstrate that patients with varying degrees of concomitant valvular disease are routinely treated in real-world practice. Restrictions were also applied to concomitant procedures and procedural access. In the surgical comparator trial DEDICATE-DZHK6 (Blankenberg et al., 2024), patients requiring additional surgical interventions, such as combined SAVR and coronary artery bypass grafting (CABG), were excluded to avoid the higher procedural risk associated with combined operations. In contrast, registry data from SWEDEHEART (Todt et al., 2026) included patients undergoing SAVR with or without concomitant CABG, reflecting standard clinical practice. Moreover, most RCTs mandated strict suitability for transfemoral access, as in PARTNER 3 (Leon et al., 2025) and RHEIA (Tchetche et al., 2025), whereas observational data from OCEAN-TAVI (Taniguchi et al., 2022) report that alternative access routes, such as transapical, trans-subclavian, and direct aortic approaches, are commonly used in patients with peripheral vascular disease.
E. Supplemental Evidence and Guidance
1. Evidence from Meta-analyses
Our search identified seven meta-analyses. The findings from these meta-analyses are consistent with our qualitative review of primary studies.
Comparison of TAVR with standard care (Surgery/clinical surveillance)
All-cause mortality
Similar to the primary studies analyzed in the current report, the included SLRs and meta-analyses demonstrate that TAVR and SAVR yield comparable survival outcomes beyond the early follow-up period, particularly at intermediate- and long-term follow-up. The current report found that across the eight RCTs, TAVR and SAVR or CS had comparable all-cause mortality, with no statistically significant differences. However, two trials reported a 1-year mortality benefit for TAVR over SAVR: one examined asymptomatic patients (Evolut Low Risk) and the other focused on low-to-intermediate-risk patients (DEDICATE-DZHK6). One trial (PARTNER 2 SAPIEN 3) reported that at one year, TAVR was significantly better than SAVR, but at five years mortality rates were similar.
Lerman et al. (2023) reported no significant difference in all-cause mortality between TAVR and SAVR at one to two years based on eight trials. Kazemian et al. (2024) also observed that mortality risks were similar between TAVR and SAVR beyond one year of follow-up. Consistent with these findings, two meta-analyses evaluating mid-term (four to five years) all-cause mortality reported similar results for TAVR and SAVR: Pascoal et al. (2026) reported comparable mid-term (four to five years) all-cause mortality between groups across six trials, and Rahman et al. (2024) found no survival difference between TAVR and SAVR at a mean follow-up of 4.3 years. In contrast, important differences emerged when examining early and intermediate-term outcomes. Kazemian et al. (2024) demonstrated that TAVR significantly reduced all-cause mortality at 30 days and between 30 days and one year compared with SAVR. Rahman et al. (2024) similarly reported a 38% relative reduction in 1-year all-cause mortality in favor of TAVR. Khan et al. (2025), analyzing 18,671 patients, concluded that TAVR was superior to SAVR, with significantly lower odds of all-cause mortality. Notably, the reported heterogeneity in the observed meta-estimates across studies typically ranged from none to low, except the 4-5-year all-cause mortality estimates in Rahman et al. (2024) and Pascoal et al. (2026), which both reflected moderate heterogeneity in mortality estimates across the included trials.
Unlike the current report, where none of the included major RCTs reported higher mortality with TAVR, Moradi et al. (2025) reported a divergence in meta-regression results over time, with lower 1-year mortality associated with TAVR but higher 5-year mortality compared with SAVR. Extending these observations, Pascoal et al. (2026) found that at five years, TAVR was associated with significantly higher all-cause mortality relative to SAVR. The substantial heterogeneity observed across studies likely reflects a combination of clinical and procedural variability, along with differences in study design, patient populations, follow-up duration, and overall methodological quality. Sensitivity analysis by Moradi et al. (2025) revealed that Arnold et al. (2021) was the primary source for high heterogeneity in the 5-year follow-up for all-cause mortality. Pascoal et al. (2026) reported a higher risk of death from non-CV causes for TAVR than SAVR in AS patients with low to moderate surgical risk, which could cause this variation.
Collectively, these findings indicate that while TAVR and SAVR demonstrate broadly similar survival in the mid-term, TAVR confers early survival advantages that may attenuate or reverse at longer-term follow-up in some analyses.
CV mortality
Similar to the primary studies analysis included in the current report, across seven meta-analyses, the evidence indicated that TAVR and SAVR were associated with largely comparable CV mortality over mid- to long-term follow-up, despite signals of early CV survival benefit with TAVR in some analyses. Collectively, these findings suggest that any early TAVR advantage tends to attenuate with longer follow-up. The current report found that across the eight RCTs, TAVR and SAVR or CS had comparable CV mortality, with no statistically significant differences. However, one trial reported a 1-year CV mortality benefit for TAVR over SAVR among the low-to-intermediate-risk population (DEDICATE-DZHK6). Another trial (PARTNER 2 SAPIEN 3) reported that at one year, TAVR was significantly better than SAVR, but at five years CV mortality rates were similar.
In the short term (30 days to one year), several meta-analysis studies reported lower CV mortality with TAVR, although results were not entirely consistent. Kazemian et al. (2024) demonstrated a significant 50% reduction in 30-day CV mortality with TAVR compared with SAVR and observed a non-significant trend toward lower CV mortality between 30 days and one year. Rahman et al. (2024) similarly reported a significant reduction in 1-year CV death, favoring TAVR. In contrast, Moradi et al. (2025) observed a non-significant difference in 1-year CV mortality between TAVR and SAVR. Khan et al. (2025) also reported similar 30-day CV mortality between groups, with numerically lower rates in the TAVR arm that did not reach statistical significance.
At mid- to long-term follow-up (≥1 year), the majority of analyses demonstrated convergence in CV mortality between TAVR and SAVR. Kazemian et al. (2024) reported comparable CV mortality beyond one year and, through meta-regression, showed that the early survival benefit of TAVR significantly diminished over time. Rahman et al. (2024) similarly found no difference in CV death at a follow-up of zero to five years. Lerman et al. (2023) observed numerically lower CV mortality with TAVR during early and mid-term follow-up (one to two years), although this difference was not statistically significant.
As with all-cause mortality, a similar trend was noted for CV mortality. Moradi et al. (2025) reported no significant differences at two years or three years, but identified a significantly higher risk of CV mortality with TAVR at five years. Pascoal et al. (2026) concluded that mid-term CV mortality was similar between TAVR and SAVR, while noting a higher risk of non-CV mortality with TAVR.
Overall, these meta-analyses suggest that TAVR may confer an early reduction in CV mortality, but this advantage is not consistently sustained over longer follow-up, with most studies demonstrating comparable CV mortality between TAVR and SAVR beyond the first year.
Stroke
Similar to the primary studies analysis included in the current report, across seven meta-analyses, the evidence indicated that TAVR and SAVR were associated with broadly comparable stroke risk over mid- to long-term follow-up, despite signals of early protection against disabling neurological events with TAVR in selected analyses. Overall, any early advantage observed with TAVR appeared to attenuate with longer follow-up.
In the current report, across eight RCTs, TAVR and SAVR/CS had comparable stroke rates, with no statistically significant differences. However, three RCTs examining patients from low- to intermediate-risk populations (PARTNER 3, PARTNER 2 SAPIEN 3, and the SURTAVI trial) reported a statistically significant reduction in stroke with TAVR compared to SAVR at early follow-up (one to two years), but at five years, stroke rates were similar. One RCT reported an increase in stroke in the TAVR group at one year (NOTION 2). Regarding disabling stroke, the current report found that nine RCTs reported that TAVR and SAVR or CS showed comparable disabling stroke, with no statistically significant differences reported. Whereas two RCTs (DEDICATE-DZHK6 and PARTNER 2 SAPIEN 3) reported statistically significant reduction in disabling stroke with TAVR compared to SAVR at 1- and 5-year follow-up.
In the short-term and early follow-up period, several studies reported favorable stroke outcomes with TAVR, particularly for disabling stroke. Khan et al. (2025), analyzing 18,671 patients, demonstrated that TAVR was superior to SAVR in reducing overall stroke risk, with significantly lower odds of stroke in the TAVR group. Kazemian et al. (2024) similarly reported a significant 63% reduction in the risk of disabling stroke within the first 30 days following TAVR, although the risk of all-cause stroke during this early period was comparable between TAVR and SAVR. At one year, Rahman et al. (2024) found no statistically significant difference in the incidence of all stroke between TAVR and SAVR. Consistent with this, Moradi et al. (2025) reported similar 1-year stroke rates between treatment strategies; however, the analyzed studies had moderately heterogeneous effect estimates, and a sensitivity analysis excluding the PARTNER 1 trial demonstrated a statistically significant reduction in disabling stroke with TAVR at one year and reduced inconsistency across study estimates.
At mid- to long-term follow-up, stroke rates converged between the two approaches. Pascoal et al. (2026) reported no significant differences between TAVR and SAVR in mid-term outcomes (≥4 years) for either all stroke or disabling stroke. Using meta-regression, Kazemian et al. (2024) demonstrated that the early absolute risk reduction in disabling stroke associated with TAVR significantly diminished over time (p = 0.009), with no significant difference observed beyond one year of follow-up. Moradi et al. (2025) further confirmed comparable long-term outcomes, reporting similar stroke rates between TAVR and SAVR at five years. Rahman et al. (2024) likewise observed nearly identical stroke incidence at a follow-up of zero to five years (6.6% for TAVR vs. 6.9% for SAVR).
Taken together, these findings suggest that while TAVR may reduce the risk of disabling stroke in the early post-procedural period, overall stroke risk is comparable between TAVR and SAVR over mid-to-long-term follow-up, with no consistent long-term neurological advantage observed for either strategy.
MI
Consistent with the primary study analyses included in the current report, seven meta-analyses demonstrated that MI incidence was comparable between TAVR and SAVR, with no statistically significant differences observed across short-, mid-, or long-term follow-up, irrespective of patient risk profile. In the current report, we found that across the 11 RCTs, TAVR and SAVR or CS-treated patients had comparable MI rates, with no statistically significant differences. In the short-term and early follow-up period (30 days to one year), multiple analyses reported numerically lower but statistically nonsignificant MI rates with TAVR. Khan et al. (2025), analyzing 18,671 patients, reported 30-day MI rates of 0.84% for TAVR and 1.13% for SAVR, corresponding to a non-significant reduction with TAVR. Similarly, Kazemian et al. (2024) observed a non-significant trend toward lower MI risk with TAVR during the first 30 days. At one year, Rahman et al. (2024) found no significant difference in MI incidence between TAVR and SAVR, a finding that was corroborated by Moradi et al. (2025), who reported similar one-year MI rates.
At mid-to-long-term follow-up, MI risk remained comparable between the two interventions. Pascoal et al. (2026) evaluated trials with at least four years of follow-up and found no significant difference in MI incidence between TAVR and SAVR. Rahman et al. (2024) similarly reported nearly identical MI rates at a follow-up of zero to five years (3.2% for TAVR vs. 3.4% for SAVR). Consistent with these findings, Lerman et al. (2023) observed no statistically significant difference in MI risk at one and two years of follow-up. Moradi et al. (2025) further confirmed the absence of divergence over time, reporting no significant differences in MI risk at two years, three years, or five years. Extending these observations, Kazemian et al. (2024) reported that MI risk remained similar between TAVR and SAVR across all follow-up intervals beyond the initial 30 days in low-risk patient populations.
Overall, these findings indicate that MI rates following AVR are consistently low and statistically similar between TAVR and SAVR, with no evidence of a sustained advantage for either strategy across varying durations of follow-up.
New permanent pacemaker implantation
Consistent with the primary study analyses included in the current report, across seven meta-analyses, new permanent pacemaker implantation consistently emerged as a clear and statistically significant disadvantage of TAVR compared with SAVR, with elevated risk observed early after the procedure and persisting through mid- and long-term follow-up in most analyses. The current report found that across the 12 RCTs, four showed comparable pacemaker implantation rates between TAVR and SAVR/CS, with no statistically significant differences. However, eight RCTs reported that the rate of new pacemaker implantation (excluding pacemakers or ICDs at baseline) was statistically significantly higher with TAVR than with SAVR at follow-up time periods ranging from one to 10 years.
In the short-term and early follow-up periods, TAVR was consistently associated with a higher risk of pacemaker implantation. Kazemian et al. (2024), analyzing 4,682 patients from six randomized trials, reported a more than threefold increase in the risk of permanent pacemaker implantation within the first 30 days following TAVR compared with SAVR. Moradi et al. (2025), pooling data from 10 RCTs, similarly found that at one year, TAVR was associated with a significantly higher risk of new pacemaker implantation. Rahman et al. (2024) corroborated these findings in an analysis of 5,122 patients, reporting markedly higher 1-year pacemaker implantation rates with TAVR compared with SAVR (14.9% vs. 6.3%).
At mid- to long-term follow-up, the risk of pacemaker implantation associated with TAVR persisted. Lerman et al. (2023), analyzing 8,780 patients, found that at two years, pacemaker implantation remained significantly more frequent in the TAVR group (17.1% vs. 9.0%; OR: 2.28). Moradi et al. (2025) provided longitudinal evidence demonstrating sustained elevation in pacemaker risk at two years, three years, and five years. Consistent with these findings, Pascoal et al. (2026), evaluating 6,444 patients with at least four years of follow-up, reported that the incidence of new pacemaker implantation remained significantly higher following TAVR. Rahman et al. (2024) further confirmed this pattern at intermediate-term follow-up (zero to five years), with substantially higher pacemaker implantation rates in the TAVR group. Meta-regression results across these SLRs demonstrated a high degree of heterogeneity in the estimated effects of treatment on pacemaker implantation (all I2 ≥ 75%), highlighting considerable variability between the included studies in the reported effect of TAVR or SAVR on this outcome, despite consistently significant findings across trials.
Notably, Kazemian et al. (2024) observed that although the risk of pacemaker implantation was markedly higher early after TAVR, differences between TAVR and SAVR became less pronounced beyond the initial 30-day period in certain analyses. Nevertheless, taken together, these findings consistently indicate that new permanent pacemaker implantation remains one of the most robust and enduring disadvantages of TAVR compared with SAVR across the evidence.
Reintervention
The current report found that across the nine RCTs, seven reported comparable reintervention rates between TAVR and SAVR/CS, with no statistically significant differences. However, two RCTs in intermediate-risk populations (PARTNER 2 and SURTAVI) reported significantly higher reintervention rates with TAVR at five years.
Across seven meta-analyses, evaluation of aortic valve reintervention revealed heterogeneous findings, including some evidence of a higher early reintervention risk following TAVR, with longer-term outcomes that generally converged and became comparable to SAVR.
In the early follow-up period, Moradi et al. (2025) reported a higher rate of aortic valve reintervention after TAVR. In an analysis of 10 RCTs, Moradi et al. (2025) reported a significantly higher reintervention rate at one year for TAVR compared with SAVR. This elevated risk persisted at two years. However, by five years, the difference was no longer statistically significant, indicating attenuation of early divergence over time (Moradi et al., 2025).
In contrast, several other analyses reported no significant differences in reintervention rates across short-, mid-, and long-term follow-up. Rahman et al. (2024), evaluating six RCTs involving 5,122 patients, found no statistically significant difference in aortic valve reintervention at one year and similarly no difference at zero to five years. Kazemian et al. (2024) also concluded, based on six randomized trials including 4,682 patients, that the risk of aortic valve reintervention was comparable between TAVR and SAVR across all follow-up intervals in low-surgical-risk populations.
Focusing on mid- to long-term outcomes, Pascoal et al. (2026) reported no significant difference in pooled mid-term rehospitalization, which frequently captures valve-related reintervention events, between TAVR and SAVR. Pascoal et al. (2026) further highlighted long-term data from the NOTION trial, where at 10 years, bioprosthetic valve failure (a composite endpoint including valve reintervention) occurred in 10.8% of TAVR patients and 15.1% of SAVR patients, a difference that did not reach statistical significance.
Overall, these findings suggest that although TAVR may be associated with a higher risk of aortic valve reintervention in the early years following implantation, reintervention rates are similar over longer-term follow-up, with no consistent evidence of inferior durability compared with SAVR in pooled analyses.
KCCQ
The current report found that across the 10 RCTs, TAVR and SAVR/CS showed greater improvement in health status, with TAVR showing greater improvement at early time points, particularly within the first month after the procedure. Long-term PROs are largely comparable to those achieved with surgery, with no statistically significant differences reported. However, only one SLR and meta-analysis reported data on KCCQ.
In the early follow-up period, Khan et al. (2025) reported that TAVR was associated with a significantly greater improvement in the KCCQ Overall Summary score at 30 days compared with SAVR. The mean difference in KCCQ-OS score change favored TAVR by 12.76 points, which the authors reported as a clinically meaningful and statistically significant early benefit. At 30 days, patients treated with TAVR experienced a substantially greater improvement in health status, with a mean change in KCCQ-OS score of 17.87, compared with 6.27 in the SAVR group (Khan et al., 2025).
These findings indicate that TAVR was associated with faster early recovery and superior short-term health status compared with SAVR, a pattern that aligns with the less invasive nature of the transcatheter approach and its reduced perioperative burden on patients.
Methodological Considerations and Potential Bias
Across the included meta-analyses, important methodological considerations may influence the interpretation of patient-reported and functional outcomes. Lerman et al. (2023) highlighted that subjective endpoints, such as quality-of-life and health status measures, are inherently susceptible to detection bias. This concern is particularly relevant because blinding of participants and clinical personnel was not feasible, given the fundamentally different procedural characteristics of surgical versus transcatheter approaches (Lerman et al., 2023). Lerman et al. (2023) emphasized that interpretation of these findings should be contextualized within these methodological limitations. In clinical practice, especially among patients at lower surgical risk, decisions regarding valve replacement strategy continue to rely heavily on clinical judgment and shared decision-making, balancing early functional benefits against long-term outcomes and procedural trade-offs.
Composite: death and disabling stroke
Similar to the mixed results of the current report, across SLRs evaluating composite outcomes, the evidence suggests that TAVR may confer an early advantage when death and disabling stroke are considered jointly, although this benefit is not consistently sustained with longer follow-up and is sensitive to the influence of individual trials.
Lerman et al. (2023) reported that TAVR was associated with a significantly lower risk of the composite endpoint of all-cause mortality or disabling stroke during mid-term follow-up, despite observing no significant difference between TAVR and SAVR for stroke alone. In a sensitivity analysis, Lerman et al. (2023) identified the UK TAVI trial as an outlier, noting that the stroke rate in the TAVR group was approximately double that observed in the SAVR group, highlighting the influence of individual studies on pooled estimates. Rahman et al. (2024) similarly demonstrated that the early benefit of TAVR for the composite endpoint of death or disabling stroke at one year was not maintained at longer-term follow-up, with no significant difference between TAVR and SAVR at five years.
Overall, these findings indicate that while composite endpoints may capture an early clinical advantage with TAVR, long-term outcomes appear comparable between TAVR and SAVR, and results may be influenced by specific trial-level effects identified through sensitivity analyses.
Comparisons of different valve types
Across multiple meta-analyses and subgroup evaluations, outcomes between SEV and BEV were largely comparable for major clinical endpoints, with consistent differences observed for conduction disturbances. Elkholy et al. (2025) reported no significant differences between SEV and BEV in all-cause or CV mortality at 30 days or one year, nor in MI or reintervention outcomes. Similarly, stroke risk did not differ significantly between valve types overall; however, individual studies showed heterogeneous results, with some reporting lower stroke rates with SEV at one year and others noting higher early disabling stroke rates with SEV (e.g., the OPERA-TAVI registry).
Subgroup analyses by Lerman et al. (2023) confirmed no significant interaction between valve type and CV mortality, MI, or stroke, reinforcing the overall comparability of clinical efficacy across TAVR platforms. However, both Elkholy et al. (2025) and Lerman et al. (2023) consistently demonstrated a significantly higher risk of permanent pacemaker implantation with SEV compared with BEV and substantially higher event rates in the SEV group (Lerman et al., 2023: 26.6% vs. 10.9%). In addition, SEV was associated with a higher incidence of moderate-to-severe paravalvular aortic regurgitation.
Longer-term analyses further indicated that MEVs may be associated with an increased risk of pacemaker implantation compared with other transcatheter systems and SAVR (Pascoal et al., 2026). Notably, advances in newer-generation devices, including SAPIEN 3 (BEV) and Evolut R/PRO (SEV), have substantially reduced pacemaker implantation rates relative to earlier valve generations (Rahman et al., 2024). Overall, while SEV and BEV demonstrate comparable performance for mortality, stroke, MI, and reintervention, differences in conduction outcomes and paravalvular regurgitation remain key distinguishing factors between valve platforms.
2. Evidence-based Guidelines / Professional Society Recommendations / Consensus Statements / Other Expert Opinion
Evidence-based Guidelines
The most current, prevailing U.S.-based professional guideline applicable to the objectives and research questions in this review was published by the American College of Cardiology and American Heart Association (ACC/AHA) Joint Committee for the management of patients with valvular heart disease (Otto et al., 2021). More recently, the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) have published updated professional recommendations in the 2025 ESC/EACTS Guidelines for the management of valvular heart disease (Praz et al., 2025). These evidence-based guidelines are focused on the diagnosis and management of adult patients with valvular heart disease and provide the class of recommendation (strength), accounting for the estimated magnitude and certainty of benefit in proportion to risk. Recommendations also include the level of evidence as a rating of the quality of scientific evidence supporting the intervention on the basis of the type, quantity, and consistency of data from clinical trials and other sources (Otto et al., 2021; Praz et al., 2025).
The ESC/EACTS guidelines note that, as of the guideline publication, no medical therapies have been shown to influence the natural history of AS, and the initiation of medical therapy or temporary improvement in symptoms should not delay intervention in symptomatic severe AS and HF patients (Praz et al., 2025). The ACC/AHA guidelines recommend treatment of severe AS should be based primarily on symptoms or reduced ventricular systolic function, whether using TAVR or SAVR (Otto et al., 2021). Earlier intervention may be considered if indicated by results of exercise testing, biomarkers, rapid progression, or the presence of very severe stenosis (Otto et al., 2021). Current guidelines with the highest strength of recommendation for an AVR are those for patients with symptomatic severe AS and for asymptomatic severe AS patients undergoing cardiac surgery for other indications or with an LVEF of <50% (Otto et al., 2021).
Decisions regarding the type of AVR approach (TAVR vs SAVR) and valve type (mechanical vs bioprosthetic) in patients with severe AS should be made through shared decision-making that considers the lifetime risks and benefits of each option (Otto et al., 2021). The ACC/AHA guidelines provide a detailed flowchart with clinical decision-making considerations for selecting valve (mechanical vs. bioprosthetic) and procedure (TAVR vs. SAVR) types (see Otto et al., 2021, p. e57, Figure 3). This decision tree should be supplemented by a shared decision-making process that accounts for the patient’s values and preferences, includes discussion of the indications for and against each approach, and addresses the potential need for and risks associated with valve reintervention (Otto et al., 2021). Likewise, the ESC/EACTS guidelines provide concise flow diagrams assisting practitioners with the management of severe AS patients (Praz et al., 2025, p 4666-4667, Figure 7 & 8) and emphasize that the mode of AV intervention depends on the patient’s estimated life expectancy, the expected prosthesis durability, patient preference, and specific trade-offs associated with different treatment options.
Although other treatment procedure options are available to AS patients (e.g., Ross procedure, balloon aortic valvuloplasty), these procedures are to be rarely considered in select patients (Otto et al., 2021; Praz et al., 2025) and are not reviewed in this report.
The ESC/EACTS guidelines comment that available data do not suggest systematic differences in durability between the two AVR treatment modalities (Praz et al., 2025). However, when both SAVR and TAVR are options, both guidelines stress consideration on the limited data about TAVR durability relative to patient life expectancy, compared with the greater than 50-year SAVR durability data, that includes specific valve types across different age groups. Multiple factors may limit direct comparison of the modalities, including potential selection and survival bias, the use of variable definitions of structural valve dysfunction, limited follow-up durations, differential attrition rates, competing risk of death, low representation of patients aged <70 years in RCTs, and the use of multiple valve types in the surgical arms of RCTs (Praz et al., 2025). Without data for the use of TAVR in patients <65 years of age when developing the guidelines, valve durability is of higher priority in younger patients, who typically have a longer life expectancy and lower surgical risk (Otto et al., 2021). This is reflected in the ACC/AHA 2020 recommendations, based on the published evidence, to recommend SAVR for adults <65 years of age unless life expectancy is limited by comorbid cardiac or noncardiac conditions (Otto et al., 2021). The ESC/EACTS guidelines acknowledge the lack of randomized data in AV patients younger than 70 years, but recommend SAVR as the preferred treatment in patients <70 years of age if surgical risk is low (Praz et al., 2025). ESC/EACTS guidelines recommend TAVR as the primary treatment modality in elderly patients ≥70 years of age with a tricuspid AV, if anatomy is suitable and transfemoral access is feasible, to reduce the risk of early adverse outcomes and accelerate recovery (Praz et al., 2025).
See Table 6, 7 and 8 in Appendix B for additional summary and comparison of these guidelines.
ACC/AHA 2020 guidelines include recommendations for the Multidisciplinary Heart Valve Team (MDT) and Heart Valve Centers (Otto et al., 2021). The guidelines issue a Class 1 (strong) recommendation that severe valvular heart disease patients should be evaluated by an MDT when intervention is considered. Likewise, the ESC/EACTS 2025 guidelines emphasize the importance of Heart Valve Centers, with institution requirements, and the value of a “Heart Team” approach (Praz et al., 2025). Both guidelines note the complexity of mixed findings related to procedural volume and clinical outcomes, including surgical complication rate and mortality rate.
Several other clinical guideline recommendations were identified for this report and are briefly outlined below.
National Institute for Health and Care Excellence (NICE) guidance on heart valve disease (NICE, 2021a; 2021b).
NICE guidance on treatment of symptomatic severe AS states that for patients at high or prohibitive risk for cardiac surgery, TAVR is recommended, whereas SAVR is recommended for patients at low or intermediate risk. For adults with asymptomatic AS, NICE guidance recommends consideration of TAVR if certain criteria are met, including thresholds related to aortic valve area, brain natriuretic peptide, exercise treadmill test, low-flow low-gradient, LVEF and maximum aortic valve jet velocity. The NICE guidelines outline the suitability for TAVR as dependent on an appropriate access for inserting the TAVR catheter, the morphology of the valve, aortic root and ascending aorta, and the degree and distribution of calcium in the aortic valve. TAVR is considered an option for 1) All people expected to have an unacceptably high risk of mortality or morbidity as a result of surgery (e.g., risk of infection in immunosuppressed patients), 2) All people expected to have unacceptably strenuous and prolonged recovery from surgery and an extended need for rehabilitation because of frailty, reduced mobility, or musculoskeletal conditions, and 3) All people with low life expectancy, either because of their age or because they have life-limiting comorbidities.
A key difference between NICE guidance documents and the ESC/EACTS and ACC/AHA guidelines is that NICE methods focus resources on interventions that have been proven to be not just clinically effective but cost-effective also. A supplement to the NICE guidelines (NICE, 2021b) note the clinical efficacy and benefits of TAVR (e.g., help reduce pressure on SAVR waiting times, less need for general anesthetic, reduced hospital stay), while also recognizing that TAVR is currently not cost effective for patients defined as intermediate or low risk for cardiac surgery for aortic valve disease. The supplement concludes with a statement that a commissioning position on TAVR that aligns with the NICE guidance will be developed once a cost-effective solution has been finalized. NICE website status indicates the review is “in progress” as of May 2026.
2019 Canadian Cardiovascular Society Position Statement for Transcatheter Aortic Valve Implantation (Asgar et al., 2019)
The Canadian Cardiovascular Society recommends that the choice for TAVR or SAVR be an individualized decision based on consideration of factors that might favor one therapy over another. The conditions that favor TAVR include risk of surgical mortality or morbidity of intermediate or greater risk (e.g., STS score ≥ 3), advanced age (> 75 years), frailty, limited mobility, small annulus requiring a small surgical valve (prosthesis size ≤ 21 mm), longevity unlikely (minimum two years required), and mediastinal anatomy unfavorable for surgery (i.e., porcelain aorta, previous thoracotomy, patent grafts, hostile root). The conditions that favor SAVR include aortic root anatomy unfavorable for TAVR, advanced atrioventricular block, especially right bundle branch block, nonfemoral access required, congenital bicuspid valve, risk of coronary obstruction or coronary access concerns, pure aortic insufficiency, concomitant conditions requiring surgery (e.g., multivalve disease), aortic aneurysm or dissection, and endocarditis. The choice between the two therapies should depend on the patient-specific risks and technical considerations. In addition, the consensus of a multidisciplinary heart team and patients’ preferences and values should be taken into account. The guidelines also provide recommendations for institutional, program, and operator requirements for performing TAVR.
Non-amyloid specific treatment for transthyretin cardiac amyloidosis: a clinical consensus statement of the ESC Heart Failure Association (Garcia-Pavia et al., 2025)
Transthyretin amyloid cardiomyopathy (ATTR-CM) is a progressive and often fatal disease that is a frequent cause of progressive heart failure. AS is common in ATTR-CM with a prevalence that ranges from 13% to 16% in candidates for TAVR. The ESC Heart Failure Association addresses the management of AS in the context of ATTR-CM, advising TAVR as the preferred treatment for these patients with both ATTR-CM and AS.
Professional Society Recommendations / Consensus Statements
Several professional society guidance documents were identified that may be relevant to clinical decision-making. Of note, one publication below was available and incorporated in the 2019 TAVR NCD reconsideration (Bavaria et al) and is included again for this reconsideration because an updated consensus statement by these entities has not been issued at the time of writing.
A) 2019 AATS/ACC/ASE/SCAI/STS expert consensus systems of care document: A proposal to optimize care for patients with valvular heart disease: A joint report of the American Association for Thoracic Surgery, American College of Cardiology, American Society of Echocardiography, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons (Nishimura et al., 2019). The Joint Committee propose an integrated model of care for valvular heart disease patients to optimize outcomes for all patients and ultimately improve the care of these patients at all centers. Use of a multidisciplinary team (MDT) and patient shared decision-making is emphasized. Recommendations for Level I and II Valve Center designations are provided. For example, a Comprehensive (Level I) Valve Center should have the resources and capabilities to evaluate and perform all commercially approved interventional and surgical procedures with advanced imaging modalities, while a Primary (Level II) Valve Center should have, at a minimum, the expertise and resources to perform transfemoral TAVR and surgical procedures, such as isolated SAVR.
B) 2024 ACC/AHA Clinical Performance and Quality Measures for Adults With Valvular and Structural Heart Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Performance Measures (Jneid et al., 2024). This report provides a set of 11 valvular heart disease measures (five performance and six quality measures), each with a strong (class 1) strength of recommendation. All measures are attributed to the individual practitioner, with one documentation measure also attributed to facilities. The Committee developed the measure set to assist health care practitioners and facilities in measuring and comparing healthcare, ultimately improving care and outcomes. The measure set is the first set of performance and quality measures for VHD and structural heart disease (SHD) that are created by the ACC and AHA in collaboration with other societies and are not all specific to AS.
C) SCAI Expert Consensus Statement on Alternative Access for Transcatheter (Sherwood et al., 2025). While transfemoral access in TAVR for AS remains the primary route due to its lower complication rates and favorable outcomes, a subset of patients has anatomical or clinical factors precluding this approach. When femoral artery access is not suitable, alternative access routes such as transaxillary, transcarotid, and transcaval provide viable options. The SCAI consensus statement recommends that extrathoracic (transcarotid, transcaval, and transaxillary/subclavian) access be selected over intrathoracic (transaortic and transapical) nonfemoral access for TAVR to reduce morbidity and mortality. Furthermore, when anatomically feasible, transcarotid or transcaval access are generally preferable to transaxillary/subclavian access. The decision of alternative access route for TAVR should be individualized to each patient based on CT evaluation of anatomical factors, patient risk factors and preferences, and multidisciplinary heart team discussions.
D) 2018 AATS/ACC/SCAI/STS expert consensus systems of care document: Operator and institutional recommendations and requirements for transcatheter aortic valve replacement: A joint report of the American Association for Thoracic Surgery, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons (Bavaria et al., 2019). The goal of the joint writing committee was to provide a quality framework for any U.S. center providing TAVR as a treatment option for AV disease. The Joint Report provides structural measures of quality that include the requirement that operators and institutions have the skills, experience, foundational TAVR and SAVR volume, and facilities that are fundamental to delivering TAVR and SAVR.
E) Valve Academic Research Consortium 3: Updated endpoint definitions for aortic valve clinical research (VARC-3 Writing Committee et al., 2021). This document provides an update of the VARC-2 guidance for the most appropriate clinical endpoint definitions to be used in the conduct of TAVR and SAVR clinical research. The VARC Writing Committee emphasized that it is crucial to assign device or procedure-relatedness to the clinical endpoints and to catalogue event timing relative to the index procedure. VARC-3 proposed clinical endpoints include: Mortality, Neurologic events, Hospitalization (or re-hospitalization), Bleeding and transfusions, Vascular and access-related complications, Cardiac structural complications, Other procedural or valve-related complications, New conduction disturbances and arrhythmias, Acute kidney injury, MI, Bioprosthetic valve dysfunction, Leaflet thickening and reduced motion, Clinically significant valve thrombosis, PRO and health status, and Composite endpoints. Each endpoint is described and further delineated. For example, when reporting Mortality, “all-cause mortality” should remain the preferred primary endpoint measure but should be further classified as CV or non-CV when possible. VARC proposed composite endpoints may be multiple endpoints related to technical success (at exit from procedure room), device success (at 30 days or in-hospital), early patient safety (at 30 days), clinical efficacy (at one year and thereafter), and valve-related long-term clinical efficacy (at five years and thereafter).
F) Minimum core data elements for evaluation of TAVR: A scientific statement by PASSION CV, HVC, and TVT Registry (Simonato et al., 2022). This report represents a comprehensive effort to produce a consensus list of 132 minimum core data elements to support more efficient, consistent, and informative TAVR device evidence for regulatory submissions, safety surveillance, best practice, and hospital quality assessments. The TAVR data elements are grouped into three domains: baseline data (demographics, comorbidities, laboratory tests, imaging), procedural data, and follow-up data (outcomes, laboratory tests, imaging).
3. Appropriate Use Criteria
ACR appropriateness criteria preprocedural planning for transcatheter aortic valve replacement: 2023 update (Expert Panels on Vascular and Cardiac Imaging et al., 2023). The American College of Radiology evidence-based guidelines focus on preprocedural planning for TAVR, evaluating the initial imaging modalities for pre-procedure planning. Two sets of guidelines are provided: assessment of aortic root and assessment of supravalvular aorta and vascular access.
This review identified a substantial body of evidence evaluating TAVR for AS, anchored primarily in RCTs and supplemented by large observational registry-based studies. In total, 17 RCTs were included for detailed analysis, encompassing approximately 10,686 patients treated with TAVR across a broad spectrum of surgical risk profiles, symptom status, and valve platforms. These trials were predominantly multicenter and multinational, with follow-up durations ranging from 30 days to 10 years, providing short, intermediate, and some long-term outcome data. Observational evidence from seven large registry-based studies contributed data on more than 450,000 patients, offering a supplementary real-world context.
Evidence from RCTs
Across RCTs in symptomatic patients, the most commonly reported outcomes included all-cause mortality, CV mortality, stroke (including disabling stroke), MI, permanent pacemaker implantation, valve reintervention, and patient-reported health status (KCCQ). Overall, the certainty of evidence was rated as moderate to high for most clinical outcomes based on GRADE criteria, with downgrades primarily driven by indirectness, inconsistency across subgroups or time points, and imprecision for less frequent events. The breakdown for specific health outcomes below applies to symptomatic patients with severe AS; the case for asymptomatic patients with severe AS is discussed separately.
Mortality Outcomes
For all-cause mortality, RCT evidence for symptomatic patients with severe AS demonstrates that TAVR provides outcomes comparable to SAVR across low-, intermediate-, and high-risk populations, with greater support for use of TAVR the higher the surgical risk, at least for the duration of the trials. The implications of longer-term follow-up of trial patients is discussed in CMS Coverage Analysis section. While a small number of trials reported early (one year) mortality benefits favoring TAVR, notably in low- and intermediate-risk patients, these advantages were generally not sustained at longer follow-up, and long-term mortality converged between treatment groups. CV mortality findings were similar, with predominantly comparable outcomes between TAVR and SAVR, with moderate-certainty evidence.
Neurologic Outcomes
RCT evidence for stroke and disabling stroke indicated no consistent, statistically-significant difference between TAVR and SAVR, although individual trials reported conflicting results at early follow-up. These discrepancies, combined with relatively low event rates and wide confidence intervals in some studies, resulted in a moderate GRADE rating for stroke-related outcomes.
MI and Reintervention
Across RCTs, MI rates were uniformly low and did not differ significantly between TAVR and SAVR, with high-certainty evidence due to consistency and narrow confidence intervals. For valve reintervention, most RCTs reported no statistically significant differences, although two intermediate-risk trials observed a higher long-term (5-year) reintervention risk following TAVR. The certainty of evidence was high with GRADE.
Pacemaker Implantation
In contrast to mortality and neurologic outcomes, new permanent pacemaker implantation consistently occurred more frequently after TAVR than SAVR across RCTs for symptomatic patients, with a clear and consistent direction of effect. This outcome was supported by high-certainty evidence, reflecting robust event counts, consistency across studies, and narrow confidence intervals. Although a small number of trials showed comparable pacemaker rates, the overall body of evidence indicates increased pacemaker implantation associated with TAVR.
Health Status and Quality of Life
PROs measured by the KCCQ were almost universally reported in RCTs. Most trials demonstrated similar long-term improvements in health status between TAVR and SAVR, while some showed greater early improvement with TAVR, typically within 30 days post-procedure. These early advantages typically attenuated over time. The GRADE assessment had overall moderate certainty due to inconsistency and imprecision.
Evidence from Meta-Analyses
Multiple recent meta-analyses evaluating TAVR across surgical risk categories were reviewed as supplemental evidence. These analyses largely reinforced the findings from primary RCTs in symptomatic patients, concluding that TAVR is noninferior to SAVR for mortality and major CV outcomes, whereas the higher pacemaker rates and stroke risk were comparable to those observed in RCTs. However, because meta-analyses frequently included overlapping trials, mixed valve generations, and heterogeneous follow-up durations, their conclusions were considered supportive rather than determinative, and the GRADE assessment was anchored primarily in the underlying RCT evidence.
Evidence from Observational and Supplemental Sources
Large observational studies, tapping registry data from the STS/ACC TVT Registry, SWEDEHEART, and OCEAN-TAVI, provided insights into real-world effectiveness, procedural evolution, and broader patient inclusion, particularly among older, frailer patients and those with multiple comorbidities who were underrepresented in RCTs. These data generally corroborated RCT findings for mortality and stroke outcomes, while highlighting greater clinical heterogeneity, wider valve-type use, and longer-term practice patterns. Although observational evidence was not formally graded, it strengthened external validity and applicability to the Medicare population.
Professional society guidelines and consensus statements consistently supported the use of AVR across expanding risk categories when delivered in experienced centers using a multidisciplinary heart team approach. However, guidelines do not provide class 1 granular recommendations regarding patient subgroups or procedural settings, underscoring ongoing evidence gaps. ACC/AHA 2020 strongly recommends TAVR in symptomatic patients with severe AS who are >80 years of age or for younger patients with a life expectancy <10 years and no anatomic contraindication to transfemoral TAVR. The guideline strongly recommends TAVR in symptomatic patients of any age with severe AS and a high or prohibitive surgical risk, if predicted post-TAVR survival is >12 months with an acceptable quality of life. The guideline strongly recommends that the choice between TAVR and SAVR be made through shared decision-making, with consideration of expected patient longevity and valve durability.
Across the reviewed evidence, limited data were available to assess the differential effectiveness and safety of TAVR across patient subgroups. Most RCTs were not specifically powered to detect treatment–subgroup interactions, and subgroup analyses were frequently exploratory, limiting the certainty of conclusions. Nonetheless, available findings suggest that overall treatment effects of TAVR versus SAVR in symptomatic patients with severe AS were generally consistent across age, sex, and surgical risk categories, with no strong or reproducible evidence of statistically significant differential impact on major outcomes for these factors.
The above discussion of RCTs and supporting observational studies applies generally to symptomatic patients with severe AS. In contrast, there has been only one large, contemporary RCT on asymptomatic patients, with controversial results (as discussed in detail in the CMS Coverage Analysis section below). We address how this evidence - for symptomatic and asymptomatic patients alike - informs our proposed decision criteria in the CMS Coverage Analysis section of this proposed decision memorandum.
Conclusions and Key Evidence Gaps
The evidence demonstrates that TAVR provides clinical outcomes comparable to SAVR across most major health endpoints, with moderate to high certainty for mortality, CV outcomes, stroke, and MI, for symptomatic patients with severe AS. In terms of safety, the most consistent difference observed was a higher risk of permanent pacemaker implantation with TAVR, which remains an important consideration in shared decision-making.
In terms of patient health outcomes for symptomatic patients with severe AS, the evidence is stronger for TAVR the higher the surgical risk. There are significant evidence gaps for asymptomatic patients generally, and especially for those with preserved LVEF. Other significant subgroups where better evidence is needed to inform the choice of treatment include patients with greater life expectancy (given that SAVR valves have durability data far exceeding that for TAVR), low surgical risk, and/or bicuspid aortic valve anatomy. In addition, for both symptomatic and asymptomatic patients with severe AS, the evidence on differential effectiveness across other patient subgroups, particularly by age, sex, race/ethnicity, and comorbidity burden, remains limited, as does guidance on optimal treatment settings beyond tertiary care hospitals.
III. Public Comment
CMS uses the initial public comments to inform its proposed decision. Public comments that cite published clinical evidence give CMS useful information. Public comments that contain information on unpublished evidence such as the results of individual practitioners or patients are less rigorous and therefore less useful for making a coverage determination.
First Comment Period: December 15, 2025 – January 14, 2026
During the first 30-day public comment period CMS received 171 comments. The majority of commenters supported some form of Medicare coverage for TAVR. All comments that were submitted during the comment period without personal health information may be viewed by using the following link: https://www.cms.gov/medicare-coverage-database/view/ncacal-public-comments.aspx?NCAId=321&bc=ACAAAAAAQAAA&=.
The majority of comments were provided by health care professionals. Seven comments were from medical technology manufacturers, including Abbott, AtriCure, Boston Scientific Corporation, Edwards Lifesciences, JenaValve Technology, Inc., Medtronic, and Pi-Cardia. Two comments were from industry organizations, AdvaMed and the Medical Device Manufacturers Association. Four comments were from professional associations, including one from the Association of Black Cardiologists, one from the Preventive Cardiovascular Nurses Association, one from the Society of Thoracic Surgeons, and a joint comment from the American Association for Thoracic Surgery, the American College of Cardiology, the Heart Failure Society of America, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. Eleven comments were from health care organizations, including Bon Secours Mercy Health, Baptist Health of South Florida Heart and Vascular Institute, Baptist Health Systems in Kentucky and Indiana, the Cardiovascular Service Line of Baylor Scott and White Health, the Corewell Health West TAVR Program, the Henry Ford Health System Center for Structural Heart Disease, the Structural Heart & Valve Center at New York Presbyterian Hospital/Columbia University Irving Medical Center, the cardiac surgeons at Northwestern Medicine, the University of Michigan Multidisciplinary TAVR Team, the University of Pennsylvania TAVR Program, and the Washington University in St. Louis Structural Team. Other comments were from Access for All, the Alliance for Aging Research, the Conservative Political Action Coalition Foundation Center for Regulatory Freedom, Consumer Action for a Strong Economy, the Global Coalition on Aging, the Heart & Valve Collaboratory, the Heart Valve Disease Policy Task Force, Heart Valve Voice US, the National Center for Health Research, the Partnership to Fight Chronic Disease, the Stanford Mussallem Center for Biodesign, the Taxpayers Protection Alliance, The Mended Hearts, Inc., WomenHeart: The National Coalition for Women with Heart Disease, the UCSF Team for High-Value Care, and the Patient, Consumer, and Public Health Coalition.
Second Comment Period: June 15, 2026 – July 15, 2026
Publication of this proposed decision initiates the second 30-day public comment period. CMS will summarize and provide detailed responses to the public comments when issuing the final decision memorandum.
IV. CMS Coverage Analysis
A. CMS Coverage Authority
National coverage determinations (NCDs) are determinations by the Secretary with respect to whether a particular item or service is covered nationally by Medicare (§ 1869(f)(1)(B) of the Social Security Act (the Act)). In general, in order to be covered by Medicare, an item or service must fall within one or more benefit categories contained within Part A or Part B and must not be otherwise excluded from coverage. Moreover, with limited exceptions, items or services must be reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member (§ 1862(a)(1)(A) of the Act).
When the available evidence is insufficient to demonstrate that the items and services are reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member under section 1862(a)(1)(A) of the Act, coverage with evidence development (CED) has been used to support evidence development for certain items and services that are likely to show benefit for the Medicare population. CED has been a pathway whereby, after a CMS and AHRQ review, Medicare covers items and services on the condition that they are furnished in the context of clinical studies or with the collection of additional clinical data (See CMS’ CED Guidance Document.) CED relies primarily on the statutory exception in section 1862(a)(1)(E) of the Act, which effectively permits Medicare payment for items and services that are reasonable and necessary to carry out research conducted pursuant to section 1142 of the Act. Section 1142 of the Act describes the authority of AHRQ to conduct and support research that appropriately reflect the needs and priorities of the Medicare program.
B. CMS Analysis of Coverage of TAVR for Aortic Stenosis
The objective of a national coverage analysis (NCA) is a critical appraisal of the evidence to determine to what degree we are confident that the specific evidence questions raised in an NCA can be answered conclusively. When conducting NCAs for an item or service under the reasonable and necessary statute, CMS generally makes three kinds of assessments, about: (1) the quality of relevant individual studies; (2) what conclusions can be drawn from the body of the evidence on the direction, magnitude, and durability of the intervention’s potential benefits and harms; and (3) the generalizability of findings from relevant studies to the Medicare beneficiary population.
As such, this NCA encompasses:
- The Evidence Questions, which inform the Literature Search, the Background, and the Evidence Review, which assesses both individual studies and the overall strength, gaps and limitations of the evidence base.
- The CMS Coverage Analysis (this section), which pulls all of this together and provides the rationale for the specific coverage criteria in the decision, based on the totality of the evidence reviewed, along with consideration of the administrative feasibility of decision criteria, and the need for consistent standards across similar NCDs.
(See CMS’ Evidence Review Guidance Document. )
In this NCA on TAVR for AS, the evidence in the Clinical Evidence Review section (Section II) indicates that there is convincing, meaningful clinical benefit for use of TAVR in certain patients with symptomatic severe AS, that is both demonstrated in clinical trials, and generalizable to the Medicare population in usual care settings. As such, we propose that TAVR is reasonable and necessary for these patients under § 1861(a)(1)(A) of the Act.
However, as identified in the Conclusions and Evidence Gaps (Section II.F.) and this Analysis below, there are questions about the clinical utility of TAVR for Medicare patients with asymptomatic AS that need to be answered before CMS would be able to determine if coverage is reasonable and necessary. The evidence for some subgroups of asymptomatic patients with AS appears promising (likely to show benefit) and therefore suitable for CED under § 1861(a)(1)(E) of the Act; for other subgroups, the evidence is too immature for inclusion in CED at this time. Additionally, at least one patient subgroup represents use of TAVR for a different disease (aortic regurgitation), and is therefore out-of-scope for this NCD on TAVR for AS.
As context, the current NCD (2019) requires:
- For coverage of FDA “on label” use for symptomatic AS, participation in a prospective, national, audited registry.
- Heart team-based care, with interventional cardiologists and surgeons (the “operators”) doing independent patient evaluations and then jointly performing each TAVR procedure.
- Minimum volume thresholds for hospitals and operators.
- Coverage of FDA “off label” use only in CMS-approved CED studies.
[ https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=N&ncaid=293&fromTracking=Y&bc=AAAAAAAAACAA&=" ]
Based on new evidence since this prior decision, we now propose, for Medicare coverage of TAVR for patients with severe AS, to:
- end CED requirements and provide coverage for treatment of symptomatic patients;
- expand coverage to asymptomatic patients under CED;
- maintain the concept and composition of the heart team; and
- streamline and update requirements related to pre-procedural patient assessments, intraoperative requirements, and operator and hospital procedural volume requirements.
The discussion below provides the rationale for our proposed patient criteria for coverage of TAVR, as well as minimal criteria for treating physicians and hospitals that we believe are necessary to achieve the clinical benefits seen in studies.
1. Rationale for Proposed Coverage Criteria
TAVR is covered for the treatment of Medicare beneficiaries with:
- Symptomatic severe AS under § 1862 (a)(1)(A) of the Social Security Act (the Act).
Rationale:
TAVR for AS has been performed in the U.S. for more than 20 years at over 860 sites and studied in over 450,00 patients. For patients with symptomatic severe AS specifically, TAVR has been studied in at least 17 RCTs with > 10,000 patients (see Evidence Review section). Early trials first evaluated patients with symptomatic severe AS who were at high risk of dying from surgical AVR. As TAVR knowledge, techniques, and technology evolved, additional RCTs compared TAVR to SAVR in intermediate-risk, then low-risk, patients (see Tables 1 and 2 in section II.D.). In parallel, the TVT registry collected similar data on > 450,000 real-world patients receiving TAVR in broader community settings. This constellation of rigorous RCTs, larger real-world registry studies, and involvement of competing companies followed a deliberate, step-by-step process of assessing the clinical utility of TAVR vs SAVR for each new subpopulation of symptomatic patients with severe AS.
The evidence from these numerous, generally well-designed RCTs and parallel real-world registry studies, reviewed in depth in the Clinical Evidence Review of this proposed decision, demonstrates that use of TAVR in appropriate patients with symptomatic severe AS meaningfully improves patient-centered health outcomes such as mortality, hospitalization, and quality of life. The figure below (see Figure 1, Patient Characteristics Favoring TAVR or SAVR as excerpted from Praz 2025 European Guidelines) identifies factors such as vascular and valve anatomy, comorbidities, and life expectancy, that impact whether TAVR or SAVR may be preferred. TAVR may also be a reasonable choice for patients eligible for either procedure; this is true even for certain low surgical risk patients and becomes increasingly so the higher the surgical risk.
Figure 1 (Praz 2025)
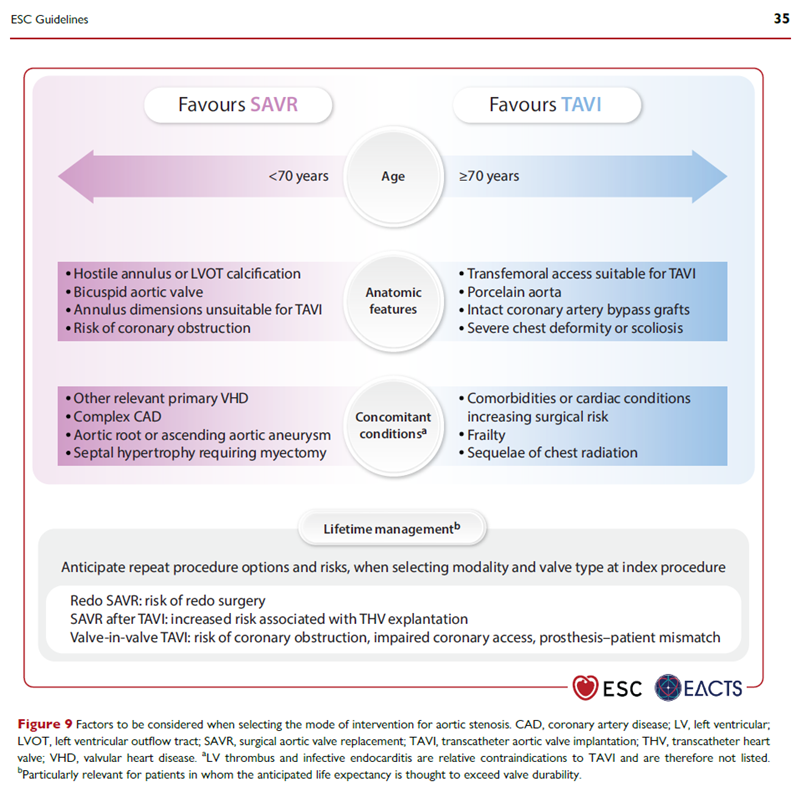
The RCT evidence cited above is the backbone for current ACC/AHA guideline class 1 recommendations for use of TAVR in patients with symptomatic severe aortic stenosis (Otto 2021). Similarly, the 2025 ESC/EACT guidelines state: “Symptomatic severe AS has an unfavourable prognosis if left untreated, and early intervention is strongly recommended in all patients with an estimated life expectancy exceeding 1 year”; this European guideline leaves to the heart team much of the decision of which procedure (TAVR or SAVR) is appropriate for a given symptomatic patient (Praz 2025).
CED Questions – Answered (for symptomatic severe AS)
In light of this evidence, we believe the CED questions posed in the 2019 TAVR NCD have been sufficiently answered for Medicare beneficiaries with symptomatic severe AS.
Q1: When performed outside a controlled clinical study, how do outcomes and adverse events compare to the pivotal clinical studies?
A1: Based on the totality of evidence extensively discussed in section II above, we believe that the constellation of landmark RCTs for each patient surgical risk group (high, intermediate, low), the recent 5-7-year follow-up data for low-risk trial patients, meta-analyses, and large, longitudinal studies of real-world patients (>450,000) at real-world TAVR centers (> 860) using TVT registry data, demonstrate generalizability of trial results to the Medicare population. A caveat on generalizability for low-risk patients has emerged since that prior NCD. A key study, “Low-Risk Patients: The Critical Divergence From RCTs” (Vekstein 2025), assessed 108,407 patients (in the TVT registry) designated low-risk by a heart team (from years 2020 to 2024), of whom 42,093 met enrollment criteria for the low-risk trials. In the heart-team designated low-risk population, 1-year outcomes included 4.6% mortality, 2.6% stroke, and 90% alive and well. For the trial-eligible population, 1-year outcomes included 3.1% mortality, 2.4% stroke, and 92% alive and well. As the study’s primary outcome, these mortality rates of 3-4.6% can be compared to 1-2% mortality in the low-risk trials (PARTNER 2 and Evolut Low Risk). The authors believe this divergence in mortality is because of greater comorbidity burden and lower baseline quality of life (captured in KCCQ scores), as well as greater fragmentation of care, for real-world patients.
This is unsurprising, as in our NCDs across medical fields we have observed lower effect generally when interventions move from rigorously controlled trials to the general population. The greater the “effect size difference” between trial intervention and control groups (in superiority trials), the more likely Medicare beneficiaries will achieve meaningful outcomes, despite some expected degradation of effect.
A similar study for SAVR using the STS Adult Cardiac Surgery Database (as the TVT registry contains only TAVR data, not SAVR) demonstrated similar mortality, and actually lower stroke rates, compared to the SAVR RCT arm (Thourani 2024). No head-to-head comparison of TAVR vs SAVR in real-world registry patients has been performed as there is no single, unified registry containing both TAVR and SAVR data (and cross-registry comparison is fraught with methodological pitfalls).
Some experts and public comments believe that evidence like the Vekstein 2025 study justifies continuing CED specifically for those symptomatic severe AS patients with low surgical risk (in addition to extending CED to asymptomatic patients and other subgroups).
However, the purpose of CED is to generate sufficient data to call the evidentiary question. That has happened, and despite inherent limitations of observational (non-randomized) studies, we believe this new data is sufficient to meaningfully inform guideline writers and heart teams alike. The heart team shared decision-making with the patient should consider, along with vascular and valve anatomy and the like, that low-risk patients will likely have better TAVR outcomes the closer they meet actual trial enrollment criteria, and even when they do meet trial criteria, they should seriously consider SAVR (unless other factors prevail). However, we believe TAVR remains a reasonable alternative to SAVR for many of these low-risk patients, and that guideline writers and heart teams could determine which procedure is better for which patient.
We believe that the totality of new evidence since our 2019 NCD supports ending CED and providing coverage for TAVR (with certain criteria) for patients with symptomatic severe AS.
Q2: What is the long-term durability of the device?
A2: While SAVR valves have demonstrated durability for >15 years, TAVR valves have RCT data out to approximately five to seven years (see section II). The PARTNER 3 trial in low-risk patients (Sapien 3, balloon-expandable valve) at 7-year follow-up demonstrates reintervention rates (because of failed valves) of 6.7% for TAVR vs 6.0% for SAVR, with no statistically significant difference (NS). The Evolut Low Risk trial (Evolut, self-expanding valve) shows rough equivalence at five years, with the reintervention curves separating after that: TAVR (SAVR) reintervention is 3.3% (2.5%) at five years (NS), 5.5% (3.3%) at six years, and 10% (6%) at seven years (a significant difference with p< 0.05, but in a post-hoc exploratory study and as such is hypothesis-generating only). These follow-up studies are new since our 2019 TAVR NCD.
Some commenters note that the NOTION trial followed patients up to 10 years. However, we believe this data is not reliable on several counts: small size (280 patients vs 1,000 in PARTNER 3, and 1,414 in EVOLUT Low Risk) at only three centers (all Scandinavian); an obsolete TAVR valve (CoreValve, self-expanding) prone to paravalvular leaks and associated with permanent pacemaker implantations; and no standardization in the SAVR valves used.
Q3: What are the long-term outcomes and adverse events?
A3: The evidence to date, including the same 5-7-year follow-up results of RCTs discussed above (PARTNER 3 and EVOLUT Low Risk) demonstrate approximate equivalence of TAVR and SAVR for key outcomes such as mortality and stroke, at least for the time period studied. For example, the Evolut Low Risk Trial showed no statistical difference for a composite of “hard” outcomes of “all-cause mortality or disabling stroke” at six years between TAVR (23.3%) and SAVR (20.4%). PARTNER 3 used a different composite for its primary outcome (which included in addition to all-cause mortality and disabling strokes, all other strokes, and rehospitalizations related to the procedure, valve, or heart failure). However, focusing on similar “hard outcomes,” for all-cause mortality there was no significant difference at five years (10.0% for TAVR vs 8.2% for SAVR) or at seven years (19.5% for TAVR vs 16.8% for SAVR, although the curves start separating here). For all stroke (which includes but is not limited to disabling stroke), there was also no significant difference at seven years (8.5% TAVR vs 8.1% for SAVR).
Commentary on the seven-year data for PARTNER 3 stated: “If we focus on the long-term hard endpoints of death and stroke that patients really care about, instead of the composite outcome including early 30-day rehospitalization, we see that SAVR appears to be better than TAVR” (Badhwar 2025). The above recorded conference statement echoes the theme published by the speaker, that low surgical risk and longer life expectancy, especially for patients with bicuspid aortic valves, tends to favor SAVR over TAVR (Mehaffey and Badhwar 2025).
As for adverse events, tradeoffs have emerged across numerous RCTs (with similar findings across observational studies). For example, SAVR consistently has a higher risk of new-onset atrial fibrillation than does TAVR, while TAVR has a higher risk of permanent pacemaker implantation (see section II).
Q4: What morbidity and procedure-related factors contribute to TAVR patient outcomes?
A4: Based on the outcomes and adverse events discussed in A3 above, in general, patients who are sicker, with greater comorbidities, and a higher risk of dying during surgery, will choose TAVR (and have better outcomes), while those who are healthier, with low surgical risk, and likelihood of living 10+ years, will likely choose SAVR, other things (such as vascular anatomy suitable for TAVR) being equal. Again, this multifactorial assessment is complex, highly patient-dependent, and must include patient preferences and appetite for competing risks.
In sum, the constellation of multiple RCTs across surgical risk groups, two 5–7-year follow-up studies in low-risk symptomatic patients, and large observational studies tapping TVT registry data, demonstrate that TAVR meaningfully improves health outcomes, and thus is reasonable and necessary, for Medicare beneficiaries with symptomatic severe AS.
TAVR is covered for the treatment of Medicare beneficiaries with:
- Asymptomatic severe AS under CED, § 1862 (a)(1)(E) of the Act.
Rationale:
The current ACC/AHA guidelines give a class 1 recommendation for use of TAVR in patients with asymptomatic severe AS and a LVEF of less than 50%, a positive treadmill stress test, or other indications for open-heart surgery (Otto 2021). These guidelines do not give a similarly high recommendation for asymptomatic patients with preserved LVEF (i.e., those with normal heart function). These guidelines were written prior to completion of the recent EARLY TAVR trial, discussed below, which focused on this specific subpopulation of asymptomatic patients. Also, the 2020 ACC/AHA guidelines are likely to be updated in late 2026 or early 2027. These European guidelines in turn state, “Intervention is recommended in asymptomatic patients with severe AS and an LVEF of < 50% without another cause” (Praz 2025). Again, whether this intervention should be TAVR or SAVR is, in these guidelines, a separate question, and depends on a number of patient factors the evidence for which, we believe, is still emerging.
EARLY TAVR
In contrast to the numerous RCTs for symptomatic patients with severe AS, there is a single, large, contemporary RCT on TAVR for asymptomatic patients – EARLY TAVR. As context, while both European (Praz 2025) and U.S. (Otto 2021) guidelines give a class 1 recommendation for use of AVR in asymptomatic severe AS that includes patients with LVEF < 50%, this is rarely applicable as < 1% of asymptomatic patients have LVEF <50% (Henkl 2012). These guidelines do not give a similarly high recommendation for asymptomatic patients with preserved LVEF (≥ 50%).
Previously, two small RCTs favored SAVR over clinical surveillance for outcomes of mortality (RECOVERY), and mortality and heart-failure hospitalization (AVATAR) (Kang 2019, Banovic 2024). However, there was no TAVR arm in either trial, and the patients were low-risk, relatively young, and had very severe AS (factors that may favor SAVR over TAVR). The EVOLVED trial in turn randomized 224 patients with asymptomatic severe AS, preserved LVEF, and myocardial fibrosis to early TAVR plus guideline-directed optimal medical therapy (OMT), or to OMT alone with clinical surveillance (Loganath 2024). Myocardial fibrosis was assessed by cardiac magnetic resonance (CMR) imaging; selection for these patients was a clinical trial enrichment strategy, as this marker of myocardial damage was thought to identify patients more likely to benefit from early intervention. This small pilot study found no significant difference between the intervention and control groups for the primary composite end point of all-cause death or unplanned AS–related hospitalization.
EARLY TAVR was designed to fill the evidence gap on the benefit of early TAVR for asymptomatic patients with preserved LVEF; it specifically challenged the existing ACC/AHA guidelines recommending monitoring of symptoms and echocardiographic surveillance every six to 12 months.
As presented above in the Clinical Evidence Review, EARLY TAVR randomized 901 patients with asymptomatic severe AS and preserved LVEF to prompt TAVR, or to close clinical surveillance at the outset. The primary outcome was a composite of death, stroke, or unplanned hospitalization for CV causes (at a median of 3.8 years). The authors reported that “a primary end-point event occurred in 122 patients (26.8%) in the TAVR group and in 202 patients (45.3%) in the clinical surveillance group” – a large, statistically-significant reduction in the primary outcome, favoring early intervention. As a further breakdown: “Death occurred in 8.4% of the patients assigned to TAVR and in 9.2% of the patients assigned to clinical surveillance, stroke occurred in 4.2% and 6.7%, respectively, and unplanned hospitalization for cardiovascular causes occurred in 20.9% and 41.7%.” The authors concluded that “a strategy of early TAVR was superior to clinical surveillance in reducing the incidence of death, stroke, or unplanned hospitalization for cardiovascular causes” (Généreux 2025).
EARLY TAVR trial data shows that the positive trial result (favoring early, pre-emptive intervention) was driven by patients in the surveillance group who crossed over in the first six months (26%) because they became symptomatic or met other pre-specified criteria for progression of disease. The trial authors state that “the percentage of patients who converted to aortic-valve replacement were 26.2% (116 patients) at 6 months, 47.2% (208 patients) at 1 year, and 71.4% (312 patients) at 2 years (Fig. S5, Kaplan-Meir estimates).” Over the 5-year trial duration, 87.0% of patients in the clinical surveillance group underwent AVR. There was no significant difference between groups in stroke and all-cause mortality over 5-year follow-up (accounting for the conversions to TAVR, in intention-to-treat analysis; Généreux 2025).
A critique (pointed out in the New England Journal of Medicine Correspondence) is that what this trial actually succeeds in demonstrating is that very close clinical monitoring – closer than what 2020 ACC/AHA clinical guidelines recommend – with prompt TAVR when needed, is safe and effective. “Accordingly, the conclusion of this trial should be that clinical surveillance of asymptomatic patients is safe, and TAVR should be performed when symptoms occur. Moreover, the strategy of initial clinical surveillance might even be superior. Bioprosthetic valves have a limited durability, and delaying TAVR has the potential to prevent repeat interventions for deterioration of structural valves” (Toggweiler 2025).
Such close monitoring would also have the benefit of avoiding unnecessary procedures; a non-trivial 13% of patients in the surveillance arm never needed TAVR over the 5-year duration of the trial, despite the very close monitoring, and possible bias to intervene inherent in the study design. However, while we understand the critics’ interpretation of what the trial actually demonstrates, we also acknowledge a key study limitation, here coming from the trial authors themselves: the trial’s “level of vigilance may not be replicated in the real world, especially in care contexts in which AS is undertreated. In addition, the availability of TAVR may have resulted in a lower threshold for conversion to aortic-valve replacement once symptoms developed” (Généreux 2025).1
Both the trial’s success (in what it actually demonstrates) and this key limitation (raising the question of consistent replicability in broader community practice) informed our proposed decision. Based on our experience in evaluating numerous cardiac (and non-cardiac) interventions, this “fully work up, then wait and watch, but much more closely” strategy is unlikely to be replicable in real-world clinical practice across Medicare’s diverse geographical settings and patients. Moreover, even some experts advocating a “wait and watch closely” strategy acknowledge (on consultation) that there are some asymptomatic patients with preserved LVEF for whom early AVR (whether TAVR or SAVR) may be the preferred option (e.g., patients with rapidly increasing gradients or severely calcified valves – and such patients were generally excluded from the EARLY TAVR trial).
Regarding asymptomatic patients as a whole, in addition to this partition based on reduced vs preserved LVEF, there are other possible clinically-relevant partitions, based on clinical and laboratory parameters, to include the specific threshold fall in systolic blood pressure on a treadmill exercise test, or rise in serum beta-type natriuretic peptide (BNP) level, or acceleration of the severity of stenosis. These also have incomplete evidence, and corresponding lower-level recommendations in guidelines. Finally, the definition of severe AS may itself be undergoing change, perhaps to include early and late severe disease; this could result in different recommendations for each subgroup, again, subject to patient-physician shared decision-making. The evidence for which asymptomatic patients would benefit from early AVR (and then which of these would benefit equally or more from TAVR compared to SAVR) is still emerging.
Other trials on asymptomatic patients are underway or planned. The largest of the ongoing new trials is The Early Valve Replacement in Severe ASYmptomatic Aortic Stenosis Study (EASY-AS). This pragmatic, multicenter, prospective, parallel-group, open RCT is taking place in Europe (predominantly the UK), Australia and New Zealand. EASY-AS randomizes approximately 2,000 patients with severe asymptomatic AS to early AVR (SAVR or TAVR, as chosen by the local care team and patient) plus OMT, or to “expectant management” (OMT alone with clinical surveillance). The primary outcome (recently amended) is a composite of cardiovascular death, stroke, and heart-failure hospitalization. This trial will likely add important information on how to better identify which treatment is better for which patients, and when, and builds in a degree of “generalizability” due to its pragmatic design.
Given the evidence base for asymptomatic patients with severe AS, we believe the rationale for coverage under CED is as follows. There is a promising base of trial evidence supporting use of TAVR in asymptomatic patients (as discussed in detail above). However, because of the variability in strength of evidence, especially for various types of asymptomatic patients (e.g., reduced and mid-range vs normal ejection fraction, congenital bicuspid vs normal tricuspid aortic valve anatomy, many vs few co-morbidities, shorter vs longer life expectancy), and to limited durability data, more data is needed to better inform heart team assessments for asymptomatic patients as a whole. CED is designed to generate research to fill gaps such as this where the evidence is promising but incomplete.
The clinical evidence for use of TAVR in asymptomatic patients with reduced LVEF may be stronger than for those with preserved LVEF. However, we propose CED (rather than coverage without CED) to encompass the subgroup with reduced LVEF in part because of the question of TAVR valve durability. For many patients, whether a TAVR valve can take them 10 years or beyond (as SAVR valves can) is a key factor for deciding between TAVR, SAVR, and clinical surveillance. The evidence for use of TAVR in asymptomatic patients with preserved LVEF is, in turn, less mature (EARLY TAVR trial).
Rationale for Other Decision criteria
FDA Indication
We propose that TAVR for AS is covered when furnished with a complete aortic valve and implantation system that has received Food and Drug Administration (FDA) premarket approval (PMA) for that system’s FDA-approved indication . . .
Rationale: This ensures alignment with current FDA indications.
Physician and Heart Team Criteria
Heart Team: The patient (preoperatively and postoperatively) is under the care of a heart team: a cohesive, multi-disciplinary team of medical professionals with a specialized focus in cardiac care. The heart team concept embodies collaboration and dedication across medical specialties to offer optimal patient-centered care. The heart team:
- Must include at least one cardiac surgeon and one interventional cardiologist experienced in the care and treatment of AS with clinical privileges at the hospital where the TAVR will be furnished; and
- May include other physicians, advanced practice clinicians, and nurses, as well as research personnel and administrators.
Rationale: In part because of the original TAVR NCD, the multidisciplinary heart team (first proposed jointly by the STS and ACC), has become the standard of care. It is integrated into nearly every major relevant trial or study, society guidelines (US, European, and others), and in clinical care in hospitals nationwide. While no public comments or published commentary object to the concept of the heart team, there are competing recommendations on how to modify the application of this concept to improve efficiency and access, while maintaining comprehensive, shared decision-making, and quality of care. Aimed at preserving this balance, we propose the following modifications to the NCD’s heart team clinical operations, focusing on the patient evaluation and volume requirements for TAVR operators.
Patient Evaluation: Suitability for surgical aortic valve replacement (SAVR), TAVR, close surveillance, or palliative care must be evaluated based on individual clinical, anatomical, and procedural characteristics, lifetime management considerations, and estimated patient life expectancy. These evaluations must be documented and made available to other heart team members, the patient, and other clinicians involved in the patient’s care as appropriate, prior to the day of the procedure. Evaluations must include:
- An initial evaluation by the heart team, which could be asynchronous using medical records to identify patient suitability for TAVR or other treatments; and
- An independent, in person evaluation by a heart team TAVR operator. This cannot be satisfied through a virtual encounter.
Rationale: Patients, along with their care team, cannot make informed shared decision-making without receiving independent perspectives on a decision that is complex and multifactorial, and may reasonably include options to receive an AVR (TAVR or SAVR, depending on patient factors), or to delay or decline any procedure in favor of close clinical surveillance and optimal medical therapy (guideline-directed medical therapy tailored to the individual patient). Note that background medical therapy would apply to all of these three options. This shared decision-making process is especially important for asymptomatic patients, as discussed earlier.
However, to improve efficiency (and hence timely access), we propose to allow triage of patients from medical chart review alone, by trained heart team staff, to identify suitability for TAVR and/or other treatments. Based on this initial assessment, the heart team could choose to have either one full, in-person evaluation by a heart team TAVR operator, or if needed, two independent evaluations, with the additional option that the second evaluation could be in-person, OR through a telehealth visit, OR through review of the medical chart and images, as determined by the heart team. Thus, there is at least one, attending-physician operator in-person exam, that cannot be done virtually. A second such in-person exam is not required but may be appropriate.
The evaluations must occur prior to the day of the TAVR procedure, with the intent of giving other members of the heart team the ability to provide input, and for the patient and their referring physician or other clinicians to have a discussion about alternative treatments, prior to going in for a procedure. This is necessary to give meaning to shared decision-making. The associated provisions for appropriate documentation and communication of these independent evaluations with other heart team members and the patient’s practitioners, and the involvement of a wide range of ancillary support personnel, are widely accepted. We preserve the local team’s flexibility in determining which ancillary personnel are involved and how.
TAVR Operator: A TAVR operator must be an interventional cardiologist or cardiac surgeon member of the heart team and:
- Perform ≥ 20 total transcatheter cardiac valve (including aortic, mitral, tricuspid, or pulmonic valve) procedures, ≥ 15 of which must be TAVR, every year; or
- Perform ≥ 40 such procedures, ≥ 30 of which must be TAVR, every two years.
Joint participation of two TAVR operators in a TAVR procedure is not required but may occur if determined appropriate by the heart team. If jointly performed, both must be TAVR operators from the heart team.
Rationale: The complex volume requirements in the original NCD, which relied in part on proxy procedures (like percutaneous coronary intervention, or PCI), were adopted out of caution for a novel procedure. These requirements were also based largely on consensus rather than evidence, as the trials were just emerging. Fourteen years later, the field has matured. For example, TAVR is now commonly taught in interventional cardiology and surgical fellowships. As such, we believe it is time to both update and streamline volume requirements.
New evidence suggests that operator volumes better predict patient outcomes than do overall hospital volumes (Kumbhani 2026). This is not surprising, as across fields, people tend to get better at something the more they do it. Also, we recognize that a couple TAVR operators at a center with overall lower volume could have higher individual volumes than many operators at a center with overall higher volumes. Thus, we propose to count TAVR (and other transcatheter cardiac valve procedures, which are generally more complex than TAVR), rather than proxies, and at the individual operator rather than hospital level.
This same paper (Kumbhani 2026) supports that there is a statistically significant difference between high-volume and low-volume categories, but not between high-volume and intermediate-volume categories. Our proposed total threshold of 20 procedures annually (or 40 every two years, to allow flexibility) falls within this intermediate group identified in this study. We believe this approximate number represents a balance between quality care and access.
Some public comments suggest that patient outcomes should now replace volume as a better measure of quality care. We believe this is, unfortunately, premature. Based on our consultations with experts leading up to our 2019 TAVR NCD, we had anticipated greater development of risk-standardized patient health outcomes, reflecting longer-term outcomes that matter to heart failure patients and are commonly used as primary endpoints in trials, such as mortality, stroke, and hospitalizations. However, the sole, validated, widely accepted health outcome is the NQF-endorsed (#3610) 30-day Risk-Standardized Morbidity and Mortality Composite Following TAVR. That outcome measure, which updated an earlier measure focused on mortality alone, is a helpful and welcome development. But while it is necessary, it is not sufficient; there is a reason the 30-day mark is never the sole primary outcome in trials. While the components of the composite outcome - death, stroke, major disabling bleeding, Stage III acute kidney injury, and moderate or severe paravalvular regurgitation - were selected based on their association with 1-year risk-adjusted outcomes, multi-year outcomes are common in trials, along with many years of follow-up to assess durability of effect and safety. Moreover, the 30-day measure is less accurate and useful the lower the surgical risk and the longer the life expectancy of the patient. Thus, we believe longer-term measures would better inform patients and physicians. Finally, some expert commenters who are aware of this outcome measure (and in some cases helped develop it), nonetheless believe that some type of volume criteria is still needed.
As for the previous NCD requirement that interventional cardiologists and surgeons jointly perform each TAVR procedure, we are now proposing flexibility for local teams to decide if there will be one TAVR operator or two, and who they will be. Thus, TAVR can be performed by a single TAVR operator (who meets TAVR operator criteria), assisted by other personnel. If the heart team determines that two attending-level TAVR operators are needed, both must be from the heart team. Thus, the following combination of TAVR operators is acceptable:
- Two heart team cardiac surgeons;
- Two heart team interventional cardiologists; or
- One heart team cardiac surgeon and one heart team interventional cardiologist.
We are aware that in contemporary practice, surgeons and interventional cardiologists alike, assisted by fellows, and/or specially-trained nurses or physician assistants, have performed TAVR in selected patients as the sole attending physician operator, with excellent results – both in the US and Europe. At the same time, we acknowledge that some patients – but not all – may benefit from having both an interventional cardiologist and a surgeon involved in the technical aspects of the procedure. We believe this level of clinical practice detail is best left to the heart team practitioners and professional society guideline writers. As with other modifications we now propose, we believe this will contribute to increased efficiency and thus patient access, without compromising care.
Other healthcare professionals, including physician trainees and ancillary personnel, may assist in the TAVR procedure as determined appropriate by the heart team and standard-of-care practice. Given the maturity of the field as a whole, TAVR operators now have much better experiential knowledge of the personnel and skillsets that are needed to support a given TAVR procedure.
Hospital Criteria
TAVR procedures must be furnished in a hospital with the appropriate infrastructure that includes but is not limited to:
- On-site structural heart interventional cardiology and cardiac surgery programs.
- A post-procedure intensive care unit with personnel experienced in managing patients who have undergone open-heart valve procedures.
- A continuous quality improvement process that assesses procedural outcomes and makes necessary programmatic adjustments to assure patient safety.
Rationale: We continue to require on-site surgical back up and intensive care facilities, but do not further specify their organizational or personnel requirements, and no longer specify volume requirements for open-heart surgeries in this NCD. A continuous quality improvement program is critical for TAVR programs to assess and adjust to optimize patient outcomes.
Given the maturity of TAVR today, there is no reason a highly experienced TAVR operator should not be able to pick up his/her entire TAVR team and stand up a new TAVR program at a new hospital, based on the operator’s and team’s past experience. Moreover, no new TAVR center needs to or should “start from scratch” as they can hire experienced operators and staff from an existing, broad and competitive market, and there is a pipeline of fellows trained in TAVR entering this market every year.
CED Study Criteria
TAVR items and services are furnished for the treatment of asymptomatic severe AS with a complete aortic valve and implantation system that has received FDA PMA for that system’s FDA-approved indication in the context of a CMS-approved CED study.
CED studies must meet requirements of section B2 (Physician and Heart Team Criteria) and B3 (Hospital Criteria), have an active, contemporaneous comparator and address at least one of the following questions:
- Does TAVR, SAVR, or close surveillance until symptom onset better improve health outcomes? This is particularly relevant for patients with lower surgical risk, longer life expectancy, preserved left ventricular ejection fraction, and bicuspid aortic valves.
- What are the long-term valve re-intervention rates of TAVR vs SAVR and does having re-interventions impact health outcomes?
- Can longer term, risk-standardized, patient-centered health outcomes replace volume criteria for TAVR operators?
Any future reconsideration of this NCD would consider answers to all of these CED questions, and the totality of extant evidence in the published, peer-reviewed medical literature, to assess whether use of TAVR improves health outcomes for Medicare beneficiaries.
Rationale: Based on the evidence gaps identified in the Clinical Evidence Review and further discussed in this CMS Coverage Analysis above, we propose the above criteria and questions for CED studies.
Active, Contemporaneous Comparator
An active comparator requires comparing the intervention group with patients receiving an established alternative treatment, using randomized controlled trials, propensity score matching, or instrumental variable methods to reduce confounding by indication and healthy initiator bias (Lund 2015; Sendor 2022). The term “contemporaneous” requires that both cohorts be assembled and followed during the same calendar or time period, preventing outcome differences caused by changes in clinical practice or treatment guidelines over time when historical controls are used (Schneeweiss 2005; Sendor 2022). This is consistent with the Medicare Evidence Development & Coverage Advisory Committee (MEDCAC) 2023 panel’s answer to Voting Question #12, which requires CED study designs to minimize confounding and bias through rigorous methods and justify any exclusion of a contemporaneous comparison group.
A registry could be an appropriate platform to collect research data as the basis for CED. Various databases, including a registry, clinical EHRs, claims data, the social security death index, and patient data from any type of study (e.g., RCT, longitudinal) could be integrated. We also recognize that registries can play important roles outside of the parsimonious answering of specific research questions to include measuring and evaluating quality of care and improving upon that care. In an era of evidence-based medicine witnessing the rise of computation, penetration of EHRs into community practice, increasing ability to share and aggregate standardized data, and emergence of powerful analytical tools, the value of continually collecting and analyzing data is self-evident.
Conclusion
In sum, based on the totality of evidence reviewed in depth in the Clinical Evidence Review section, and considering public comments and expert consultations, we now propose, for Medicare coverage of TAVR for patients with severe AS, to:
- end CED requirements and provide coverage for treatment of symptomatic patients;
- expand coverage to asymptomatic patients under CED;
- maintain the concept and composition of the heart team; and
- streamline and update requirements related to pre-procedural patient assessments, intraoperative requirements, and operator and hospital procedural volume requirements.
We believe these modifications balance improved access and efficiency with maintaining safety and quality care, for patients with severe AS.
2. Evidence Questions - Answered
Our initial literature search and review of the evidence on the clinical utility of TAVR for Medicare beneficiaries with AS were guided by the three questions below. Answers to these questions inform the overarching question of whether TAVR meets the reasonable and necessary standard under § 1862(a)(1)(A) of the Act.
Q1: Is the evidence sufficient to conclude that TAVR meaningfully improves health outcomes for Medicare beneficiaries with AS?
Symptomatic severe AS: Yes
As discussed in detail above, evidence from many well-designed RCTs and real-world registry studies demonstrates that TAVR for the treatment of symptomatic severe AS meaningfully improves patient-centered health outcomes. We believe this evidence has addressed the four CED questions posed in the 2019 NCD, which supports termination of CED for this patient population. Careful consideration of patient characteristics, like vascular and valve anatomy, comorbidities and life expectancy, are critical to optimizing outcomes for AS treatment, and highlight the important role the heart team plays in shared decision-making with patients. When TAVR procedures are furnished in the context of heart team shared decision-making, by TAVR operators and in hospitals that meet the proposed requirements above, TAVR for the treatment of symptomatic severe AS is reasonable and necessary under § 1862(a)(1)(A) of the Act.
Asymptomatic severe AS: No
Evidence addressing TAVR for asymptomatic severe AS is significantly less mature than evidence supporting TAVR for symptomatic severe AS. As discussed in detail above, there is a promising base of evidence supporting the use of TAVR in asymptomatic patients from the EARLY TAVR trial. However, more data is needed to fill evidence gaps that remain for this population. The following limitations of the current evidence preclude us from answering this evidence question with ‘yes’:
- EARLY TAVR is the sole, large RCT, and there is a much smaller evidence base overall than there is for symptomatic severe AS.
- EARLY TAVR did not directly compare TAVR to SAVR in low-risk patients who are earlier in the course of disease – this is important when considering valve durability and longer life expectancy.
- EASY AS, a much larger RCT, is ongoing, with results expected in 2030-31. These results, along with longer term follow-up from EARLY TAVR and potential future studies will likely generate evidence to better inform asymptomatic AS treatment.
- Close clinical surveillance remains a strategy for many patients to safely postpone valve replacement considering the evidence gap in longer-term TAVR valve durability data.
Accordingly, we do not believe coverage of TAVR for the treatment of asymptomatic severe AS is reasonable and necessary under § 1862(a)(1)(A) of the Act. However, because the evidence base is promising and continues to develop, we are proposing to support ongoing research and cover TAVR for the treatment of asymptomatic severe AS under CED, § 1862(a)(1)(E) of the Act, when procedures are performed in CMS-approved CED studies.
Q2: Do specific characteristics or comorbidities make patients more or less likely to benefit from TAVR?
Symptomatic severe AS: Yes
Based on the evidence review and discussion above, we believe the evidence base for symptomatic severe AS is mature and comprehensive enough to inform physicians and patients engaged in shared decision-making to identify the appropriate treatment, TAVR or alternatives, given patient characteristics including comorbidities. Treatment decisions must be centered on and tailored to each patient to optimize outcomes. Extensive and longer-term data on TAVR in symptomatic severe AS patients provide critical information for making these individualized treatment decisions.
Asymptomatic severe AS: No
Similar to the response for Q1, we find that the evidence base is not robust enough to adequately inform shared decision-making between the heart team and patients in the asymptomatic population. The evidence is promising, but we have identified key evidence gaps that must be addressed to better inform treatment options and decision-making. We are proposing that CED studies can be designed to accomplish this goal and build out the evidence base to better assure the right patient receives the right treatment at the right time for asymptomatic severe AS.
Q3: Are specific treatment conditions necessary to achieve TAVR health outcomes similar to those demonstrated in the clinical studies reviewed in this analysis?
Symptomatic severe AS: Yes
We have proposed requirements for hospitals and heart teams, including TAVR operators, that we believe establish treatment conditions for patients to support optimal TAVR health outcomes based on the evidence base for symptomatic severe AS. Outcomes have strengthened over time in real-world settings and are comparable to those seen in highly prescriptive clinical studies, supporting less restrictive treatment conditions. While some requirements, like the hospital and physician procedural volume requirements, have been relaxed since the original 2012 NCD, we believe our proposals reflect the maturity of TAVR in terms of technology, procedural techniques, and training in contemporary practice. We continue to believe hospitals must have sufficient infrastructure including on-site structural heart interventional cardiology and cardiac surgery programs and intensive care units to support TAVR cases varying in complexity and potential complications. Additionally, as procedural volume requirements are relaxed and the use of TAVR continues to grow, we believe it is critical for hospitals to have a continuous quality improvement process to support necessary programmatic changes and patient safety.
Asymptomatic severe AS: Uncertain
Because the evidence base for TAVR for symptomatic severe AS is extensive, we expect the treatment conditions likely convey to TAVR for asymptomatic severe AS, but ongoing research and information generated from CED studies on this population will more clearly address this. Therefore, we believe it is appropriate to apply the same hospital and heart team requirements to TAVR for asymptomatic severe AS.
For an item or service to be covered by the Medicare program, it must fall within one of the statutorily defined benefit categories outlined in §1812 (Scope of Part A); §1832 (Scope of Part B); or §1861(s) (Definition of Medical and Other Health Services) of the Act.
TAVR qualifies as:
- Inpatient hospital services
- Physicians’ services
Note: This may not be an exhaustive list of all applicable Medicare benefit categories for this item or service.
As discussed above, we believe the CED questions posed in the 2019 TAVR NCD have been sufficiently answered for Medicare beneficiaries with symptomatic severe AS. Because the questions have been answered, we are proposing to terminate CED for Medicare beneficiaries with symptomatic severe AS under this NCD. Ongoing studies that were previously approved under CED for TAVR had been determined to meet requirements for, and are approved under, either section B4 of this NCD or the Investigational Device Exemption (IDE) regulations (42 CFR § 405 Subpart B). Ongoing studies, as specified on clinicaltrials.gov, will either continue to be posted to the CMS website of approved TAVR CED studies or will be moved to the CMS website of approved IDE studies upon finalization of this NCD.
E. Shared Decision-Making
CMS recognizes the importance of shared decision-making in many clinical scenarios and has required shared decision-making in other NCDs (for example, implantable cardiac defibrillators: https://www.cms.gov/medicare-coverage-database/details/ncd-details.aspx?NCDId=110). CMS supports clinician-patient shared decision-making for TAVR for AS, but recognizes that there is no fully developed tool available at this time. CMS strongly encourages standardized decision aids or tools. The National Quality Forum (NQF) has published standards for decision aids (www.qualityforum.org/Projects/c-d/Decision_Aids/Final_Report.aspx) to facilitate the decision-making process between a patient and physician and will be monitoring this space closely.
In July 2021, the NQF Cardiovascular Standing Committee evaluated a new TAVR measure against the NQF’s standard evaluation criteria and recommended endorsement, which was upheld by the Consensus Standards Approval Committee. The endorsed measure is NQF #3610 30-Day Risk-Standardized Morbidity and Mortality Composite Following Transcatheter Aortic Valve Replacement (TAVR), and the measure steward is the ACC. The measure “estimates hospital risk-standardized site differences for five endpoints (death from all causes, stroke, major or life-threatening bleeding, acute kidney injury, and moderate or severe paravalvular aortic regurgitation) within 30 days following transcatheter aortic valve replacement (TAVR) using the Society of Thoracic Surgeons (STS)/American College of Cardiology’s (ACC) Transcatheter Valve Therapy (TVT) Registry.” https://digitalassets.jointcommission.org/api/public/content/2ab3e5f1395440c88671859cb7b62a8d?v=cb4c901f
The above NQF-endorsed measure #3610 updated and built upon an earlier measure, NQF #3534 — 30-Day All-Cause Risk-Standardized Mortality Odds Ratio Following TAVR. Likely created in the 2019–2020 cycle, this earlier measure also tapped the STS/ACC TVT Registry, but focused on mortality only. The newer measure #3610 above adds stroke, major bleeding, acute kidney injury, and paravalvular aortic regurgitation to mortality.
https://digitalassets.jointcommission.org/api/public/content/2ab3e5f1395440c88671859cb7b62a8d?v=cb4c901f
V. History of Medicare Coverage
A. Previous National Coverage Analysis
CMS has conducted two previous National Coverage Analyses on TAVR, originally establishing the NCD (20.32) in 2012, providing coverage under CED and updating it in 2019, which continued CED but updated some coverage criteria and requirements. The current NCD requires:
- For coverage for on-label use for symptomatic AS, participation in a prospective, national, audited registry is required.
- To date, one registry has received CMS approval, the Society of Thoracic Surgeons (STS)/American College of Cardiology (ACC) Transcatheter Valve Therapy (TVT) Registry.
- Heart team-based care, with interventional cardiologists and surgeons (the “operators”) doing independent patient evaluations and then jointly performing each TAVR procedure.
- Minimum volume thresholds for hospitals and operators.
- Coverage of off-label use in CED studies only.
- Since 2012, CMS has approved 44 TAVR CED studies.
B. Current National Coverage Request
This is a reconsideration of NCD 20.32 Transcatheter Aortic Valve Replacement (TAVR). This reconsideration was externally initiated. CMS received a complete, formal request to open a reconsideration of the topic from Edwards Lifesciences. The request letter is available at https://www.cms.gov/files/document/id321.pdf.
C. Timeline of NCA Milestones
| Date | Milestone |
|---|
| December 15, 2025 |
CMS posts a tracking sheet announcing the opening of the NCA reconsideration. The first 30-day public comment period begins. |
| January 14, 2026 |
First public comment period ends. CMS receives 171 comments. |
| June 15, 2026 |
CMS posts proposed Decision Memorandum. Second 30-day public comment period begins. |
VI. Appendices
Appendix A: Proposed Medicare National Coverage Determinations Manual Language
Draft
We are seeking public comments on the proposed language that we would include in the Medicare National Coverage Determinations Manual. This proposed language does not reflect public comments that will be received on the proposed decision memorandum, and which may be revised in response to those comments.
Table of Contents
(Rev.)
20.32 - Transcatheter Aortic Valve Replacement (TAVR) for Aortic Stenosis
A. General
Transcatheter aortic valve replacement (TAVR - also known as TAVI or transcatheter aortic valve implantation) is used in the treatment of aortic stenosis. A bioprosthetic valve is inserted percutaneously using a catheter and implanted in the orifice of the aortic valve.
B. Nationally Covered Indications
The Centers for Medicare & Medicaid Services (CMS) covers transcatheter aortic valve replacement (TAVR) for severe aortic valve stenosis (or aortic stenosis (AS)) when furnished with a complete aortic valve and implantation system that has received Food and Drug Administration (FDA) premarket approval (PMA) for that system’s FDA-approved indication, and the following conditions are met.
1. Patient Criteria
TAVR is covered for the treatment of Medicare beneficiaries with:
- Symptomatic severe AS under § 1862(a)(1)(A) of the Social Security Act (the Act).
- Asymptomatic severe AS under coverage with evidence development (CED), § 1862(a)(1)(E) of the Act.
Provisions in B2 and B3 below apply to all TAVR procedures furnished under the NCD; provision B4 applies only to TAVR procedures furnished under CED.
2. Physician and Heart Team Criteria
Heart Team: The patient (preoperatively and postoperatively) is under the care of a heart team: a cohesive, multi-disciplinary team of medical professionals with a specialized focus in cardiac care. The heart team concept embodies collaboration and dedication across medical specialties to offer optimal patient-centered care. The heart team:
- Must include at least one cardiac surgeon and one interventional cardiologist experienced in the care and treatment of AS and each with clinical privileges at the hospital where the TAVR will be furnished; and
- May include other physicians, advanced practice clinicians, and nurses, as well as research personnel and administrators.
Patient Evaluation: Suitability for surgical aortic valve replacement (SAVR), TAVR, close surveillance, and palliative care must be evaluated based on individual clinical, anatomical, and procedural characteristics, lifetime management considerations, and estimated patient life expectancy. These evaluations must be documented and made available to other heart team members, the patient, and other clinicians involved in the patient’s care as appropriate, prior to the day of the procedure. Evaluations must include:
- An initial evaluation by the heart team, which could be asynchronous using medical records to identify patient suitability for TAVR or other treatments; and
- An independent, in person evaluation by a heart team TAVR operator. This cannot be satisfied through a virtual encounter.
TAVR Operator: A TAVR operator must be an interventional cardiologist or cardiac surgeon member of the heart team and:
- Perform ≥ 20 total transcatheter cardiac valve (including aortic, mitral, tricuspid, or pulmonic valve) procedures, ≥ 15 of which must be TAVR, every year; or
- Perform ≥ 40 such procedures, ≥ 30 of which must be TAVR, every two years.
Joint participation of two TAVR operators in a TAVR procedure is not required but may occur if determined appropriate by the heart team. If jointly performed, both must be TAVR operators from the heart team.
3. Hospital Criteria
TAVR procedures must be furnished in a hospital with the appropriate infrastructure that includes but is not limited to:
- On-site structural heart interventional cardiology and cardiac surgery programs.
- A post-procedure intensive care unit with personnel experienced in managing patients who have undergone open-heart valve procedures.
- A continuous quality improvement process that assesses procedural outcomes and makes necessary programmatic adjustments to assure patient safety.
4. CED Study Criteria
TAVR items and services are furnished for the treatment of asymptomatic severe AS with a complete aortic valve and implantation system that has received FDA PMA for that system’s FDA-approved indication in the context of a CMS-approved CED study.
CED studies must meet requirements of sections B2 (Physician and Heart Team Criteria) and B3 (Hospital Criteria), have an active, contemporaneous comparator and address at least one of the following questions:
- Does TAVR, SAVR, or close surveillance until symptom onset better improve health outcomes? This is particularly relevant for patients with lower surgical risk, longer life expectancy, preserved left ventricular ejection fraction, and bicuspid aortic valves.
- What are the long-term valve re-intervention rates of TAVR vs SAVR and does having re-interventions impact health outcomes?
- Can longer term, risk-standardized, patient-centered health outcomes replace volume criteria for TAVR operators?
CMS-approved CED studies must adhere to the following scientific standards (criteria 1-17 below) that have been identified by the Agency for Healthcare Research and Quality (AHRQ) as set forth in Section VI of CMS’ Coverage with Evidence Development Guidance Document, published August 7, 2024 (the “CED Guidance Document”).
- Sponsor/Investigator: The study is conducted by sponsors/investigators with the resources and skills to complete it successfully.
- Milestones: A written plan is in place that describes a detailed schedule for completion of key study milestones, including study initiation, enrollment progress, interim results reporting, and results reporting, to ensure timely completion of the CED process.
- Study Protocol: The CED study is registered with ClinicalTrials.gov and a complete final protocol, including the statistical analysis plan, is delivered to CMS prior to study initiation. The published protocol includes sufficient detail to allow a judgment of whether the study is fit-for-purpose and whether reasonable efforts will be taken to minimize the risk of bias. Any changes to approved study protocols should be explained and publicly reported.
- Study Context: The rationale for the study is supported by scientific evidence and study results are expected to fill the specified CMS-identified evidence deficiency and provide evidence sufficient to assess health outcomes.
- Study Design: The study design is selected to safely and efficiently generate valid evidence of health outcomes. The sponsors/investigators minimize the impact of confounding and biases on inferences through rigorous design and appropriate statistical techniques. If a contemporaneous comparison group is not included, this choice should be justified, and the sponsors/investigators discuss in detail how the design contributes useful information on issues such as durability or adverse event frequency that are not clearly answered in comparative studies.
- Study Population: The study population reflects the demographic and clinical diversity among the Medicare beneficiaries who are the intended population of the intervention, particularly when there is good clinical or scientific reason to expect that the results observed in premarket studies might not be observed in older adults or subpopulations identified by other clinical or demographic factors.
- Subgroup Analyses: The study protocol explicitly discusses beneficiary subpopulations affected by the item or service under investigation, particularly traditionally underrepresented groups in clinical studies, how the inclusion and exclusion requirements effect enrollment of these populations, and a plan for the retention and reporting of said populations in the trial. In the protocol, the sponsors/investigators describe plans for analyzing demographic subpopulations as well as clinically-relevant subgroups as identified in existing evidence. Description of plans for exploratory analyses, as relevant subgroups emerge, are also included.
- Care Setting: When feasible and appropriate for answering the CED question, data for the study should come from beneficiaries in their expected sites of care.
- Health Outcomes: The primary health outcome(s) for the study are those important to patients and their caregivers and that are clinically meaningful. A validated surrogate outcome that reliably predicts these outcomes may be appropriate for some questions. Generally, when study sponsors propose using surrogate endpoints to measure outcomes, they should cite validation studies published in peer-reviewed journals to provide a rationale for assuming these endpoints predict the health outcomes of interest. The cited validation studies should be longitudinal and demonstrate a statistical association between the surrogate endpoint and the health outcomes it is thought to predict.
- Objective Success Criteria: In consultation with CMS and AHRQ, sponsors/investigators establish an evidentiary threshold for the primary health outcome(s) so as to demonstrate clinically meaningful differences with sufficient precision.
- Data Quality: The data are generated or selected with attention to provenance, bias, completeness, accuracy, sufficiency of duration of observation to demonstrate durability of health outcomes, and sufficiency of sample size as required by the question.
- Construct Validity: Sponsors/investigators provide information about the validity of drawing warranted conclusions about the study population, primary exposure(s) (intervention, control), health outcome measures, and core covariates when using either primary data collected for the study about individuals or proxies of the variables of interest, or existing (secondary) data about individuals or proxies of the variables of interest.
- Sensitivity Analyses: Sponsors/investigators will demonstrate robustness of results by conducting pre-specified sensitivity testing using alternative variable or model specifications as appropriate.
- Reporting: Final results are provided to CMS and submitted for publication or reported in a publicly accessible manner within 12 months of the study’s primary completion date. Wherever possible, the study is submitted for peer review with the goal of publication using a reporting guideline appropriate for the study design and structured to enable replication. If peer-reviewed publication is not possible, results may also be published in an online publicly accessible registry dedicated to the dissemination of clinical trial information such as ClinicalTrials.gov, or in journals willing to publish in abbreviated format (e.g., for studies with incomplete results).
- Sharing: The sponsors/investigators commit to making study data publicly available by sharing data, methods, analytic code, and analytical output with CMS or with a CMS-approved third party. The study should comply with all applicable laws regarding subject privacy, including 45 CFR § 164.514 within the regulations promulgated under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and 42 CFR, Part 2: Confidentiality of Substance Use Disorder Patient Records.
- Governance: The protocol describes the information governance and data security provisions that have been established to satisfy Federal security regulations issued pursuant to HIPAA and codified at 45 CFR Parts 160 and 164 (Subparts A & C), United States Department of Health and Human Services (HHS) regulations at 42 CFR, Part 2: Confidentiality of Substance Use Disorder Patient and HHS regulations at 45 CFR Part 46, regarding informed consent for clinical study involving human subjects. In addition to the requirements under 42 CFR and 45 CFR, studies that are subject to FDA regulation must also comply with regulations at 21 CFR Parts 50 and 56 regarding the protection of human subjects and institutional review boards, respectively.
- Legal: The study is not designed to exclusively test toxicity or disease pathophysiology in healthy individuals, although it is acceptable for a study to test a reduction in toxicity of a product relative to standard of care or an appropriate comparator. For studies that involve researching the safety and effectiveness of new drugs and biological products aimed at treating life-threatening or severely-debilitating diseases, refer to additional requirements set forth in 21 CFR § 312.81(a).
Consistent with section 1142 of the Act, AHRQ supports clinical research studies that CMS determines meet all the criteria and standards identified above.
The principal investigator must submit the complete study protocol including the statistical analysis plan, identify the relevant CMS research question(s) that will be addressed, cite the location of the detailed analysis plan for those questions in the protocol, provide a statement addressing how the study satisfies each of the standards of scientific integrity (1. through 17. listed above), and the investigator's contact information, to the address below. The information will be reviewed, and approved studies will be identified on the CMS Website.
Director, Coverage and Analysis Group
Re: TAVR CED
Centers for Medicare & Medicaid Services (CMS)
7500 Security Blvd., Mail Stop S3-02-01
Baltimore, MD 21244-1850
Email address for protocol submissions: clinicalstudynotification@cms.hhs.gov
Email subject line: “CED [NCD topic (i.e. TAVR)] [name of sponsor/primary investigator]”
C. Nationally Non-covered Indications
N/A
D. Other
In addition to the national coverage described above, Medicare Administrative Contractors (MACs) may make reasonable and necessary determinations under section 1862(a)(1)(A) for any other beneficiary seeking coverage for TAVR for AS. This NCD does not apply to use of TAVR in emergency scenarios.
Nothing in this NCD precludes coverage of TAVR for AS through NCD 310.1 (Clinical Trial Policy) or through the Investigational Device Exemption (IDE) Policy.
Appendix B: Referenced Materials and Supplemental Information
II Clinical Evidence Review
B. FDA
Table 1. Timeline of TAVR Device Approvals to Date
Table 1
| Approval Date | Device | Symptomatic/Asymptomatic Indication | Implant Site | Indication Risk Stratum |
|---|
| 11/02/2011 |
Edwards SAPIEN |
Symptomatic |
Native |
Inoperable
(transfemoral access only) |
| 10/19/2012 |
Edwards SAPIEN |
Symptomatic |
Native |
High risk
(transfemoral access only) |
| 09/23/2013 |
Edwards SAPIEN |
Symptomatic |
Native |
Alternate access labeling expansion |
| 01/17/2014 |
Medtronic CoreValve |
Symptomatic |
Native |
Extreme risk |
| 06/12/2014 |
Medtronic CoreValve |
Symptomatic |
Native |
High risk |
| 06/16/2014 |
Edwards SAPIEN XT |
Symptomatic |
Native |
High risk and above |
| 03/30/2015 |
Medtronic CoreValve |
Symptomatic |
Valve-in-valve (aortic TV-in-SV) |
High risk and above |
| 06/17/2015 |
Edwards SAPIEN 3 |
Symptomatic |
Native |
High risk and above |
| 10/09/2015 |
Edwards SAPIEN XT |
Symptomatic |
Valve-in-valve (aortic TV-in-SV) |
High risk and above |
| 08/18/2016 |
Edwards SAPIEN XT |
Symptomatic |
Native |
Intermediate risk |
| 08/18/2016 |
Edwards SAPIEN 3 |
Symptomatic |
Native |
Intermediate risk |
| 06/05/2017 |
Edwards SAPIEN 3 |
Symptomatic |
Valve-in-valve (aortic and mitral TV-in-SV) |
High risk and above |
| 07/10/2017 |
Medtronic CoreValve, CoreValve Evolut R, and CoreValve PRO |
Symptomatic |
Native |
Intermediate risk |
| 04/23/2019 |
Boston Scientific Corporation LOTUS Edge Valve System |
Symptomatic |
Native |
High risk and above |
| 08/16/2019 |
Medtronic CoreValve Evolut R, Medtronic CoreValve Evolut PRO |
Symptomatic |
Native |
Low risk |
| 08/16/2019 |
Edwards SAPIEN 3, Edwards SAPIEN 3 Ultra |
Symptomatic |
Native |
Low risk |
| 09/09/2020 |
Edwards SAPIEN 3 and SAPIEN 3 Ultra |
Symptomatic |
Valve-in-valve (aortic TV-in-TV) |
High risk and above |
| 09/17/2021 |
Abbott Portico |
Symptomatic |
Native |
High risk and above |
| 08/28/2025 |
Medtronic Evolut PRO+, Medtronic Evolut FX, Medtronic Evolut FX+ |
Symptomatic |
Valve-in-valve (aortic TV-in-TV) |
High risk and above |
| 04/30/2025 |
Edwards SAPIEN 3, SAPIEN 3 Ultra, and SAPIEN 3 Ultra RESILIA |
Asymptomatic |
Native |
Low risk and above |
TV-in-SV: transcatheter valve-in-surgical valve; TV-in-TV: transcatheter valve-in-transcatheter valve
D. Review of Evidence from Primary Studies
1. Study Characteristics
Table 2. Geographical locations of the included studies
| Study/Trial Name |
Geographic Locations |
References (Author, Year) |
Randomized Controlled Trials |
| Medtronic CoreValve US High-Risk Pivotal Trial |
United States |
Arnold et al., 2021 |
| PARTNER 2 SAPIEN 3 Intermediate-Risk |
United States |
Madhavan et al., 2023 |
| EARLY TAVR |
United States, Canada |
Généreux et al., 2025 |
| PARTNER 3 |
United States, Canada |
Leon et al., 2021; Mack et al., 2023; Leon et al., 2025 |
| PARTNER 2 cohort A |
United States, Canada |
Makkar et al., 2020; Chen et al., 2020 |
| SURTAVI |
United States, Canada, Europe |
Van Mieghem et al., 2022; Amrane et al., 2019 |
| GALILEO |
United States, Canada, Europe |
Okuno et al., 2022 |
| REPRISE III |
United States, Canada, Europe, Australia |
Feldman et al., 2018; Reardon et al., 2019b; Rizik et al., 2022 |
| SMART |
United States, Canada, Europe, Middle East |
Herrmann et al., 2024; Tchétché et al., 2024 |
| Evolut Low Risk Trial |
United States, Australia, Canada, France, Japan, Netherlands, New Zealand |
Merhi et al., 2022; Forrest et al., 2022; Forrest et al., 2023 |
| PORTICO IDE |
United States, Australia |
Makkar et al., 2020b |
| DEDICATE-DZHK6 |
Germany |
Blankenberg et al., 2024 |
| SOLVE TAVI |
Germany |
Thiele et al., 2020; Feistritzer et al., 2025 |
| CHOICE |
Germany |
Abdel-Wahab et al., 2020 |
| NOTION |
Denmark, Sweden, Norway, Finland, Iceland |
Søndergaard et al., 2019; Thyregod et al., 2019; Thyregod et al., 2024 |
| NOTION-2 |
Denmark, Sweden, Norway, Finland, Iceland |
Jørgensen et al., 2024 |
| RHEIA Trial |
Various European countries |
Tchetche et al., 2025; Eltchaninoff et al., 2025 |
Observational Studies |
| STS/ACC TVT Registry (health status) |
United States |
Huded et al., 2023 |
| STS/ACC TVT Registry (temporal change analysis) |
United States |
Arnold et al., 2024 |
| LRT (Low Risk TAVR trial) |
United States |
Waksman et al., 2018 |
| OCEAN-TAVI registry |
Japan |
Taniguchi et al., 2022 |
| OBSERVANT study |
Italy |
Barbanti et al., 2019 |
| SWEDEHEART registry |
Sweden |
Todt et al., 2026 |
| RESPOND Study |
Europe, New Zealand, Latin America (extension cohort: Netherlands, UK, Poland) |
Van Mieghem et al., 2019 |
Note: References include publications that are RCTs or derived from RCTs
3. Quality of Evidence from Primary Studies
Quality rating of individual publications
For RCTs:
Using the U.S. Preventive Services Task Force (USPSTF) Criteria for Assessing Internal Validity of Individual Studies, the study quality is assessed using seven key criteria. First, the initial assembly of comparable groups should involve adequate randomization, including allocation concealment, and ensure that potential confounders are equally distributed among groups. Second, the maintenance of these comparable groups must be addressed, including aspects like attrition, cross-overs, adherence, and contamination. Third, the study should report on any important differential loss to follow up or account for the high overall loss to follow-up. Fourth, measurements must be equal, reliable, and valid, including the use of masked outcome assessments. Fifth, interventions need to be clearly defined. Sixth, all important outcomes should be considered. Lastly, the analysis should adjust for potential confounders in cohort studies or apply intention-to-treat (ITT) analysis in RCTs.
Based on these criteria, study ratings are classified as Good, Fair, or Poor. A Good rating is assigned when all criteria are met: comparable groups are assembled and maintained, follow-up is at least 80%, measurements are reliable and applied equally, interventions are clearly defined, all key outcomes are considered, and confounders are appropriately handled (including use of ITT analysis in RCTs). A Fair rating applies if some concerns exist, such as small differences in follow-up groups, acceptable but not optimal measurement instruments, partial consideration of outcomes, or incomplete adjustment for confounders, without any critical flaws. A Poor rating is given when there are major flaws, such as non-comparable or poorly maintained groups, use of unreliable or invalid measurement instruments (or lack of equal application), inadequate attention to confounders, or failure to use ITT analysis in RCTs.
For observational studies:
To evaluate the quality of a study, seven criteria are considered. First, the initial assembly of comparable groups is assessed by determining whether potential confounders were appropriately considered, either restricted or measured for later adjustment in the analysis, and whether inception cohorts were used. Second, the maintenance of comparability among groups is evaluated, including attention to attrition, crossovers, adherence, and contamination. Third, the study is assessed for important differential loss to follow-up or overall high loss to follow-up. Fourth, the quality of measurements is examined, ensuring they are equal, reliable, and valid, and whether outcome assessments were masked. Fifth, the clarity of the interventions' definition is evaluated. Sixth, it is important that all relevant outcomes are considered. Lastly, for cohort studies, appropriate statistical adjustment for potential confounders is necessary.
Based on these criteria, studies are rated as “Good,” “Fair,” or “Poor.”
A “Good” rating is assigned when all criteria are met groups are initially comparable and remain so throughout (with at least 80% follow-up); measurements are valid and applied equally; interventions are clearly defined; all important outcomes are addressed; and confounders are appropriately adjusted for in the analysis. A study is rated “Fair” if there are concerns, such as modest group imbalances after follow-up, the use of acceptable but suboptimal measurement tools, and partial consideration of outcomes or confounders, yet without any fatal flaw. A “Poor” rating is given when any fatal flaw is present, such as a lack of comparability in groups at baseline or follow-up, unreliable or non-equivalent measurement instruments, failure to mask outcome assessment, or neglect of key confounders.
Table 3: USPSTF rating for the reviewed RCT publications
| Author year |
Final rating |
| Merhi et al., 2022 |
Fair: Description of randomization method and concealment of allocation were NR; attrition NR |
| Genereux et al., 2025 |
Good: The study was well conducted regarding the criteria assessed |
| Leon et al., 2021 |
Fair: Disproportionate withdrawal between arms; ITT was not performed |
| Mack et al., 2023 |
Fair: Disproportionate withdrawal between arms; ITT was not performed |
| Leon et al., 2025 |
Fair: Disproportionate withdrawal between arms; ITT was not performed |
| Forrest et al., 2022 |
Fair: Disproportionate withdrawal between arms; ITT was not performed |
| Forrest et al., 2023 |
Fair: Disproportionate withdrawal between arms; ITT was not performed |
| Søndergaard et al., 2019 |
Fair: Randomization method NR; 3 conversions of procedure from TAVR to SAVR; Echocardiographic measurements were not adjudicated by an echocardiography core lab. All outcome measurements were made unblinded |
| Thyregod et al., 2019 |
Fair: Randomization method NR; Cross-over cases occurred in both groups; echocardiographic measurements were reported by sites and evaluated by senior cardiologists. All outcome measurements were done unblinded |
| Thyregod et al., 2024 |
Fair: Randomization method NR; Cross-over cases occurred in both groups; echocardiographic measurements were reported by sites and evaluated by senior cardiologists; All outcome measurements were done unblinded |
| Jørgensen et al., 2024 |
Fair: Randomization method NR; Cross-over cases occurred in both arms |
| Blankenberg et al., 2024 |
Fair: High proportions of withdrawals, and there were cases of crossover |
| Makkar et al., 2020 |
Fair: Imbalances in withdrawals and LTFU cases between groups |
| Madhavan et al., 2023 |
Fair: This is a post-hoc analysis with PSM; LTFU between arms was higher in TAVR patients |
| Van Mieghem et al., 2022 |
Fair: The study was well conducted, except for the imbalance in withdrawals between groups |
| Amrane et al., 2019 |
Fair: The proportion of withdrawals was imbalanced between groups |
| Thiele et al., 2020 |
Good: The study was well conducted according to the criteria assessed |
| Feistritzer et al., 2025 |
Fair: LTFU was imbalanced between groups |
| Arnold et al., 2021 |
Fair: High proportions of missing data at 5-year analysis |
| Feldman et al., 2018 |
Good: The study was well conducted according to the criteria assessed |
| Reardon et al., 2019b |
Good: The study was well conducted, according to the criteria assessed |
| Rizik et al., 2022 |
Good: The study was well conducted, meeting the criteria assessed |
| Abdel-Wahab et al., 2020 |
Good: The study was well conducted, according to the criteria assessed |
| Makkar et al., 2020b |
Good: The study was well conducted, according to the criteria assessed |
| Herrmann et al., 2024 |
Good: The study was well conducted according to the criteria assessed |
| Tchétché et al., 2024 |
Fair: There were cases of crossovers and considerable missing data |
| Tchetche et al., 2025 |
Fair: ITT was not performed |
| Eltchaninoff et al., 2025 |
Fair: ITT was not performed; LTFU and withdrawals were not reported in the pooled analysis |
| Okuno et al., 2022 |
Fair/poor: Trial was not focused on valve/type and procedure of interest, but drugs administered after TAVR. The trial was terminated early due to safety concerns; the planned sample size was not reached. The baseline characteristics of the two arms (by valve type) were unbalanced; an ITT analysis was not performed |
Abbreviations: ITT: Intention-to-treat; LTFU: Lost to follow-up; NR: Not reported; PSM: Propensity-score model; RCT: Randomized controlled trial; SAVR: Surgical aortic valve replacement; TAVR: Transcatheter aortic valve replacement
Table 4: USPSTF rating for the reviewed Observational studies
| Author year |
Final rating |
| Huded et al., 2023 |
Fair: The study was well conducted according to the criteria assessed, although the brand of devices implanted was NR; and PSM and IPW were conducted to decrease selection bias, and multiple imputation was carried out for missing data |
| Taniguchi et al., 2022 |
Fair: Missing data and LTFU were NR; incomplete information on the types/models of valves implanted |
| Arnold et al., 2024 |
Fair: IPW and IPW techniques were used; although the brand of devices implanted was NR |
| Barbanti et al., 2019 |
Fair: The study was well conducted according to the criteria assessed, although the adjudication of events was NR |
| Todt et al., 2026 |
Fair: The design was non-comparable and descriptive which limits the interpretation of findings beyond temporal trends |
| Van Mieghem et al., 2019 |
Fair: There was only one cohort of patients (no comparison), and significant LTFU for echocardiographic data (not the primary outcome) |
| Waksman et al., 2018 |
Fair: A historical cohort was used; PSM and IPW were carried out to make the groups more comparable |
Abbreviations: IPW: Inverse probability weighting; LTFU: Lost to follow-up; NR: Not reported; PSM: Propensity-score model
Summary of Assigned USPSTF Quality Ratings
RCTs
Most publications were rated fair to good quality in the USPSTF assessment, reflecting appropriate randomization, adequate baseline comparability between treatment groups, prespecified endpoints, and clear definitions of interventions and outcomes, including PARTNER 3 (Leon et al., 2021; Leon et al., 2025), Evolut Low Risk (Popma et al., 2019; Forrest et al., 2022; Forrest et al., 2023), SURTAVI (Van Mieghem et al., 2022), PARTNER 2 (Makkar et al., 2020; Madhavan et al., 2023), NOTION (Søndergaard et al., 2019; Thyregod et al., 2019; Thyregod et al., 2024), EARLY TAVR (Généreux et al., 2025), REPRISE III (Feldman et al., 2018; Reardon et al., 2019b), and DEDICATE-DZHK6 (Blankenberg et al., 2024). The follow-up duration was sufficient to assess short- to mid-term clinical outcomes, and outcome ascertainment was largely complete and reliable, supporting internal validity. As reflected in the USPSTF assessments (see Table 3 above), the majority of trials had a low risk of major selection bias and a consistent direction of effect across primary endpoints.
However, several systematic limitations were noted across RCTs:
Lack of Blinding and Performance Bias: Across nearly all RCTs, blinding of participants and treating clinicians was not feasible due to the nature of TAVR and SAVR procedures, introducing potential performance and ascertainment bias, particularly for subjective or PRO as noted in PARTNER 3 (Leon et al., 2021; Leon et al., 2025), SURTAVI (Van Mieghem et al., 2022), EARLY TAVR (Généreux et al., 2025), REPRISE III (Feldman et al., 2018), and DEDICATE-DZHK6 (Blankenberg et al., 2024).
Restrictive Eligibility Criteria and Limited Generalizability: restrictive inclusion criteria, particularly in low- and intermediate-risk populations, limit extrapolation of findings to higher-risk, frailer, or more anatomically complex patients. This limitation was highlighted in PARTNER 3 (Leon et al., 2021; Leon et al., 2025), Evolut Low Risk (Popma et al., 2019; Forrest et al., 2022), SURTAVI (Van Mieghem et al., 2022), EARLY TAVR (Généreux et al., 2025), REPRISE III (Feldman et al., 2018), and LRT (Waksman et al., 2018).
Attrition, Missing Data, and Survivorship Bias: Some trials experienced differential loss to follow-up at longer time points, which may affect the precision of late-outcome estimates. Long-term follow-up analyses were affected by incomplete echocardiographic data, or survivorship bias, particularly for functional and quality-of-life outcomes, as described in NOTION 10-year follow-up (Thyregod et al., 2024), Arnold et al., 2021 (PARTNER health status analysis), and extended analyses of Evolut Low Risk (Forrest et al., 2023).
Use of Early-Generation Valve Technology: Several RCTs evaluated early-generation transcatheter valves, which are no longer representative of contemporary practice, thereby reducing external validity. NOTION trial (Søndergaard et al., 2019; Thyregod et al., 2019; Thyregod et al., 2024) was conducted during an early phase of TAVR adoption (enrollment beginning in 2009) and used first-generation self-expanding CoreValve and early balloon-expandable SAPIEN devices. These valves lacked contemporary design features such as outer sealing skirts, optimized frame geometry, and refined delivery systems, which are now known to reduce paravalvular leak, vascular complications, and permanent pacemaker implantation. Consequently, long-term outcomes reported in NOTION may not accurately reflect results achievable with current-generation TAVR systems. PARTNER 2 cohort A (Makkar et al., 2020) evaluated TAVR using the SAPIEN XT valve, an earlier balloon-expandable platform that has since been replaced by newer devices (e.g., SAPIEN 3) incorporating improved sealing skirts and lower-profile delivery systems. The use of SAPIEN XT is associated with higher rates of paravalvular regurgitation and vascular complications than those observed with current devices, thereby limiting the applicability of the PARTNER 2 findings. REPRISE III (Feldman et al., 2018; Reardon et al., 2019b) compared a MEV with SEV. This valve platform is no longer widely used in clinical practice and differs substantially from modern BEVs and SEVs in deployment mechanics, radial force, and interaction with the conduction system.
Limited Power for Rare or Long-Term Outcomes: Many RCTs were not powered to detect differences in less frequent outcomes (e.g., stroke subtypes, MI, valve reintervention) or to draw definitive conclusions at extended follow-up. The Evolut Low Risk Trial (Forrest et al., 2023) was powered for a composite primary endpoint at earlier follow-up but had limited statistical power to detect differences in individual low-frequency events, including disabling versus non-disabling stroke, MI, and valve reintervention at extended follow-up. As event rates declined over time, confidence intervals widened, limiting the ability to draw definitive conclusions beyond the primary endpoint. Similarly, NOTION 2 (Jørgensen et al., 2024) enrolled a relatively modest sample size, which constrained the trial’s ability to reliably detect differences in infrequent clinical outcomes, such as MI, stroke subtypes, and valve reintervention. Several endpoints showed numerically different event rates but were accompanied by wide confidence intervals, indicating imprecision rather than equivalence. DEDICATE-DZHK6 (Blankenberg et al., 2024) was not powered to assess differences in individual secondary outcomes, including stroke, MI, and reintervention, particularly beyond short-term follow-up. The low absolute number of events limited inferential strength and precluded robust subgroup analyses. The SMART (Herrmann et al., 2024) focused on selected anatomical and procedural criteria and was powered primarily for its prespecified primary endpoint, resulting in insufficient power to detect differences in uncommon ischemic outcomes, including MI and stroke subtypes. Extended follow-up analyses were further limited by small event counts.
Noninferiority Design and Statistical Considerations: Several RCTs employed noninferiority designs, with limitations related to margin selection and interpretability, including REPRISE III (Feldman et al., 2018), PARTNER 3 (Leon et al., 2021), and SURTAVI (Van Mieghem et al., 2022).
Post Hoc and Subgroup Analyses: Some findings were derived from post hoc or subgroup analyses, increasing the risk of type I error and limiting inference, as noted in Amrane et al., 2019 (SURTAVI substudy), Okuno et al., 2022, and valve-specific analyses within the PARTNER 2 SAPIEN 3 cohort (Madhavan et al., 2023).
Overall, the RCT evidence base for TAVR in AS is methodologically sound and suitable for comparative effectiveness assessment, but interpretation should account for lack of blinding, evolving device technology, and limited power for uncommon or long-term outcomes.
Observational studies
Large observational studies were generally rated fair quality in the USPSTF assessment (see Table 4 above) due to their nonrandomized design, but were recognized for strong external validity, large sample sizes, and real-world applicability, including the STS/ACC TVT Registry (Huded et al., 2023), SWEDEHEART registry (Todt et al., 2026), and OCEAN-TAVI registry (Taniguchi et al., 2022). Several studies leveraged national or multinational registries with standardized data collection and adjudication of clinical outcomes, thereby enhancing reliability and completeness, as demonstrated in analyses of the STS/ACC TVT Registry (Huded et al., 2023) and SWEDEHEART (Todt et al., 2026). The observational studies employed appropriate statistical adjustment for baseline differences, using multivariable modeling or propensity score methods.
Nevertheless, several key limitations were noted in the observational studies:
Confounding and Selection Bias: All observational studies were subject to residual confounding from nonrandomized treatment allocation, even when multivariable adjustment or propensity score methods were applied. Selection bias was common because treatment allocation was based on clinical judgment rather than randomization. Treatment selection was influenced by patient risk, anatomy, frailty, and institutional practice patterns, introducing confounding by indication, particularly in comparisons between TAVR and SAVR in Huded et al., 2023, and Taniguchi et al., 2022 (OCEAN-TAVI).
Incomplete Adjustment for Clinical Complexity: Despite statistical adjustment, observational studies were limited in their ability to fully account for unmeasured confounders, such as frailty severity, cognitive impairment, operator experience, and center volume. Certain studies lacked granular anatomical or procedural detail (e.g., valve-sizing rationale, calcification burden), limiting the interpretability of outcomes related to stroke and pacemaker implantation, as noted by Taniguchi et al. (2022).
Data Completeness and Outcome Ascertainment: Registry-based studies were subject to missing data, variable follow-up completeness, and potential misclassification of exposure or outcomes, particularly for nonfatal events, as noted in analyses of the STS/ACC TVT Registry (Huded et al., 2023). Some outcomes, including stroke subtypes and cause-specific mortality, were not uniformly adjudicated across sites or over time, limiting precision in SWEDEHEART (Todt et al., 2026) and OCEAN-TAVI (Taniguchi et al., 2022).
Temporal and Technological Heterogeneity: Observational studies often spanned long enrollment periods during which TAVR technology, operator experience, and procedural techniques evolved, complicating the interpretation of pooled outcomes over time, as noted in Huded et al. (2023) and Todt et al. (2026). Earlier registry cohorts included patients treated with older-generation valves, limiting applicability to current practice when interpreting longer-term outcomes in OCEAN-TAVI (Taniguchi et al., 2022).
Follow-up Duration and Long-Term Outcomes: While registries enabled assessment of large populations, long-term follow-up was inconsistent, with attrition and variable follow-up intervals, limiting conclusions regarding valve durability, late stroke, and reintervention in Huded et al., 2023, and Todt et al., 2026. Survivor bias was present in analyses of patient-reported or functional outcomes, as these endpoints could be assessed only among patients alive and available for follow-up, as noted by Taniguchi et al. (2022).
Overall, while observational studies provide valuable real-world insights and complement the RCT evidence, particularly for broader patient populations and uncommon outcomes, their findings should be interpreted cautiously due to confounding, selection bias, and variability in data completeness.
Quality rating of the evidence from Publications derived from RCTs according to GRADE domains for outcomes
Table 5: Quality rating according to GRADE domains for outcomes
| GRADE |
Judgement |
Quality of the evidence |
Outcome: All-cause Mortality |
| Publication Study design |
28 publications |
High |
| Risk of bias |
Twenty-six (93%) publications initially assembled comparable groups and used adequate randomization. Twenty-one (75%) publications had low losses to follow-up with losses balanced between groups. Sixteen (57%) performed intention-to-treat analysis. |
High |
| Indirectness |
Overall, the patients, interventions, and comparators in the studies provide mostly direct evidence for the research question regarding the use of TAVR and improvements in health outcomes among Medicare beneficiaries compared with the standard of care. Eighteen (64%) publications compared patients undergoing TAVR with those undergoing SAVR. Nine (32%) publications compared patients with different valve types undergoing TAVR. One (4%) publication (Genereux 2025) compared TAVR with clinical surveillance. |
Moderate |
| Imprecision |
The total number of patients included in the 28 publications was 15,954, ranging from 280 to 2,032. The average sample size of the papers was 938. With a few exceptions, confidence intervals were not wide. |
High |
| Inconsistency |
The direction and magnitude of effect varied across the different trials. Overall, the results showed predominantly no statistically significant difference between the groups with regard to all-cause mortality, with 89% of publications reporting non-significant results. Three publications (Merhi 2022; Blankenberg 2024; Madhavan 2023) reported a statistically significant reduction in all-cause mortality among the TAVR group compared with the SAVR group. |
High |
| Publication bias |
Publication bias is not strongly suggested, because studies with both statistically significant and non-significant results were published, and the search for studies was comprehensive. In addition, the average sample size as 938. (If all results come from small studies, publication bias may be present.) |
High |
Outcome: Cardiovascular Mortality |
| Publication Study design |
20 publications |
High |
| Risk of bias |
Nineteen (95%) publications initially assembled comparable groups and used adequate randomization. Eighteen (90%) publications had low losses to follow-up, with losses balanced between groups. Eleven (55%) performed intention-to-treat analysis. |
High |
| Indirectness |
Overall, the patients, interventions, and comparators in the studies provide mostly direct evidence for the research question regarding the use of TAVR and improvements in health outcomes among Medicare beneficiaries compared with the standard of care. Fourteen (70%) publications compared patients undergoing TAVR with those undergoing SAVR. Five (25%) publications compared patients with different valve types undergoing TAVR. One (5%) publication (Genereux 2025) compared TAVR with clinical surveillance. |
Moderate |
| Imprecision |
The total number of patients included in the 20 publications was 13,343, ranging from 280 to 2,032. The average sample size of the publications was 1,026. With a few exceptions, confidence intervals were not wide. |
High |
| Inconsistency |
The direction and magnitude of effect varied across the different trials. Overall, the results showed no statistically significant difference between patients undergoing TAVR and those undergoing SAVR with respect to cardiovascular mortality, with 89% of publications reporting comparable results. Two publications reported a statistically significant reduction in cardiovascular mortality among the TAVR group compared with the SAVR group, ranging from HR=0.47 (95% CI=0.24-0.86) (Blankenberg 2024) to HR=0.57 (95% CI=0.38-0.87, p=0.008) (Madhavan 2023). |
High |
| Publication bias |
Publication bias was not strongly suspected, because studies with both statistically significant and non-significant results were published, and the search for studies was comprehensive. In addition, the average sample size was 1,026. (If all results come from small studies, publication bias may be present.) |
High |
Outcome: Stroke |
| Publication Study design |
23 publications |
High |
| Risk of bias |
Twenty-one (91%) publications initially assembled comparable groups and used adequate randomization. Eighteen (78%) publications had low losses to follow-up, with losses balanced between groups. Thirteen (57%) performed intention-to-treat analysis. |
High |
| Indirectness |
Overall, the patients, interventions, and comparators in the studies provide mostly direct evidence for the research question regarding the use of TAVR and improvements in health outcomes among Medicare beneficiaries compared with the standard of care. Fourteen (61%) publications compared patients undergoing TAVR with those undergoing SAVR. Eight (36%) publications compared patients with different valve types undergoing TAVR. One (5%) publication (Genereux 2025) compared TAVR with clinical surveillance. |
Moderate |
| Imprecision |
The total number of patients included in the 23 publications was 14,488 ranging from 280 to 2,032. The average sample size was 966. The majority of publications (68%) reported non-significant results. Five (23%) publications had confidence interval widths greater than 5, while the remaining reported confidence intervals that were not very wide. |
Moderate |
| Inconsistency |
The direction and magnitude of effect varied across the different trials. Overall, the results showed predominantly no statistically significant difference between the groups being compared with regard to stroke. However, three publications reported a statistically significant reduction in stroke among TAVR compared to SAVR (Leon 2021; Madhavan 2023; Van Mieghem 2022) while one publication reported an increase (Jorgensen 2024). |
High |
| Publication bias |
Publication bias was not strongly suspected, because studies with both statistically significant and non-significant results were published, and the search for studies was comprehensive. In addition, the average sample size was 966. (If all results come from small studies, publication bias may be present.) |
High |
Outcome: Disabling Stroke |
| Publication Study design |
21 publications |
High |
| Risk of bias |
Twenty (95%) publications initially assembled comparable groups and used adequate randomization. Seventeen (81%) publications had low losses to follow-up, with losses balanced between groups. Eleven (52%) performed intention-to-treat analysis. |
High |
| Indirectness |
Overall, the patients, intervention and comparators in the studies mostly provide direct evidence to the research question related to the use of TAVR and improvement of health outcomes among Medicare beneficiaries when compared to the standard of care. Fourteen (67%) publications examined TAVR compared to SAVR. Six (29%) publications compared patients with different valve types undergoing TAVR. One (5%) publication (Genereux 2025) compared TAVR with clinical surveillance. |
Moderate |
| Imprecision |
The total number of patients included in the 21 publications was 13,032 ranging from 370 to 2,032. The average sample size was 1,086. The majority of trials reported non-significant results. All reported confidence interval widths were fairly narrow (i.e., less than 2). |
High |
| Inconsistency |
Overall, the results showed predominantly no statistically significant difference between patients undergoing TAVR and those undergoing SAVR with regard to disabling stroke. However, two publications reported a statistically significant reduction in disabling stroke among TAVR compared to SAVR, ranging from HR=0.42 (95% CI=0.19-0.88) (Blankenberg 2024) to HR=0.66 (95% CI=0.43-1.00, p=0.046) (Madhavan 2023). |
High |
| Publication bias |
Publication bias was not strongly suspected, because studies with both statistically significant and non-significant results were published, and the search for studies was comprehensive. In addition, the average sample size was 1,086. (If all results come from small studies, publication bias may be present.) |
High |
Outcome: MI |
| Publication Study design |
21 publications |
High |
| Risk of bias |
Eighteen (86%) publications initially assembled comparable groups and used adequate randomization. Sixteen (76%) publications had low losses to follow-up with losses balanced between groups. Twelve (57%) performed intention-to-treat analysis. |
High |
| Indirectness |
Overall, the patients, interventions, and comparators in the studies provide mostly direct evidence for the research question regarding the use of TAVR and improvements in health outcomes among Medicare beneficiaries compared with the standard of care. Six (29%) publications compared patients with different valve types undergoing TAVR. One (5%) publication (Genereux 2025) compared TAVR with clinical surveillance. |
Moderate |
| Imprecision |
The total number of patients included in the 20 RCTs was 10,829 ranging from 280 to 2,032. The average sample size of the RCTs was 902. Reported confidence intervals were not very wide; all RCTs had confidence interval widths less than 3. |
High |
| Inconsistency |
All of the trials reported no significant difference in myocardial infarction among the TAVR group compared to the SAVR group. |
High |
| Publication bias |
Publication bias was not strongly suspected, because studies with statistically non-significant results were published, and the search for studies was comprehensive. In addition, the average sample size was 902. (If all results come from small studies, publication bias may be present.) |
High |
Outcome: New Permanent Pacemaker |
| Publication Study design |
25 publications |
High |
| Risk of bias |
Twenty-four (96%) publications initially assembled comparable groups and used adequate randomization. Nineteen (76%) publications had low losses to follow-up with losses balanced between groups. Fifteen (60%) performed intention-to-treat analysis. |
High |
| Indirectness |
Overall, the patients, intervention and comparators in the studies mostly provide direct evidence to the research question related to the use of TAVR and improvement of health outcomes among Medicare beneficiaries when compared to the standard of care. Fifteen (60%) publications compared patients undergoing TAVR with those undergoing SAVR. Nine (36%) publications compared patients with different valve types undergoing TAVR. One (4%) publication (Genereux 2025) compared TAVR with clinical surveillance. |
Moderate |
| Imprecision |
The total number of patients included in the 25 RCTs was 14,698, ranging from 280 to 2,032. The average sample size of the RCTs was 919. Reported confidence intervals for relative measures of comparison were not wide. |
High |
| Inconsistency |
The direction of effect did not vary across the different trials and was consistent across all studies, reporting higher pacemaker implantation rates in the TAVR groups except for one publication (Généreux, 2025). With the exception of five publications (Leon 2021; Mack 2023; Leon 2025; Makkar 2020; Eltchaninoff 2025), all other publications comparing TAVR with SAVR or clinical surveillance demonstrated a statistically significantly higher rate of permanent pacemaker implantation among patients undergoing TAVR. |
High |
| Publication bias |
Publication bias was not strongly suspected, because studies with both statistically significant and non-significant results were published, and the search for studies was comprehensive. In addition, the average sample size was 919. (If all results come from small studies, publication bias may be present.) |
High |
Outcome: Reintervention |
| Publication Study design |
20 publications |
High |
| Risk of bias |
Nineteen (95%) publications initially assembled comparable groups and used adequate randomization. Sixteen (80%) publications had low losses to follow-up with losses balanced between groups. Ten (50%) performed intention-to-treat analysis. |
High |
| Indirectness |
Overall, the patients, intervention and comparators in the studies mostly provide direct evidence to the research question related to the use of TAVR and improvement of health outcomes among Medicare beneficiaries when compared to the standard of care. Fifteen (75%) publications compared patients undergoing TAVR compared with those undergoing SAVR. Five (25%) publications (Feldman 2018, Rizik 2022, Reardon 2019, Tchetche 2024, Herrmann 2024) compared patients with different valve types undergoing TAVR. |
Moderate |
| Imprecision |
The total number of patients included in the 20 publications was 11,241, ranging from 280 to 2,032. The average sample size was 1,124. Except in a few studies, reported confidence intervals for relative measures of comparison were not wide (i.e., less than 2). |
High |
| Inconsistency |
With the exception of two publications, all RCTs showed no statistically significant difference in frequency of reintervention between TAVR and SAVR. Two publications reported significantly against TAVR, indicating a higher risk of reintervention. The PARTNER 2 cohort A trial showed a 5-year hazard ratio of 3.28 (95% CI: 1.32 to 8.13), significantly favoring SAVR for aortic valve reintervention (Makkar 2020). Similarly, the SURTAVI trial showed a significantly increased risk of reintervention at 5 years in the TAVR group (HR 2.21, 95% CI: 1.10 to 4.45) (Van Mieghen 2022). |
High |
| Publication bias |
Publication bias was not strongly suspected, because both statistically significant and non-significant studies were published, and the search for studies was comprehensive. In addition, the average sample siz was 1,124. (If all results come from small studies, publication bias may be present.) |
High |
Outcome: KCCQ |
| Publication Study design |
16 publications |
High |
| Risk of bias |
Fifteen (94%) publications initially assembled comparable groups and used adequate randomization. Eleven (69%) publications had low losses to follow-up with losses balanced between groups. Eight (50%) performed intention-to-treat analysis. |
High |
| Indirectness |
Overall, the patients, intervention and comparators in the studies mostly provide direct evidence to the research question related to the use of TAVR and improvement of health outcomes among Medicare beneficiaries when compared to the standard of care. Eleven (69%) publications compared patients undergoing TAVR with those undergoing SAVR. Four (25%) publications (Makkar 2020b, Rizik 2022, Tchetche 2024, Herrmann 2024) compared patients with different valve types undergoing TAVR. One (5%) publication (Genereux 2025) compared TAVR with clinical surveillance. |
Moderate |
| Imprecision |
The total number of patients included in the 16 publicaitons was 11,477 ranging from 370 to 2,032. The average sample size was 956. When reported, confidence intervals were fairly wide (e.g., greater than 5). |
Moderate |
| Inconsistency |
10 publications reported no statistically significant difference in change in KCCQ scores between TAVR and SAVR from baseline to the end of follow-up, while six demonstrated significantly greater KCCQ improvement with TAVR over SAVR/CS, typically evident at early follow-up (e.g., 1 month) and attenuating over longer-term follow up (Merhi 2022, Eltchaninoff 2025, Généreux 2025; Leon 2021, Arnold 2021, Tchetche 2025). |
High |
| Publication bias |
Publication bias was not strongly suspected, because both statistically significant and non-significant studies were published, and the search for studies was comprehensive. In addition, the average sample size was 979. (If all results come from small studies, publication bias may be present.) |
High |
Note: GRADE assessment was performed for outcomes from RCTs; no assessment was performed for the composite outcomes given varied outcome definitions across studies.
E. Supplemental Evidence and Guidance
2. Evidence-based Guidelines / Professional Society Recommendations / Consensus Statements / Other Expert Opinion
Table 6. ACC/AHA 2020 & ESC/EACTS 2025 clinical guideline recommendations for timing of intervention (TAVR; SAVR) in AS patients
| ACC/AHA 2020 |
|
|
ESC/EACTS 2025 |
|
|
| Patient Assessment |
COR |
LOE |
Patient Assessment |
COR |
LOE |
| Moderate AS who are undergoing cardiac surgery for other indications. |
2b Weak: AVR may be considered |
C-EO |
Symptomatic & asymptomatic patients with moderate AS (AVA of 1.0–1.5 cm2 or mean aortic gradient of 25–40 mmHg) in normal-flow conditions undergoing CABG or surgical intervention on the ascending aorta. |
IIa: SAVR should be considered |
C |
| Asymptomatic severe AS patients who are undergoing cardiac surgery for other indications. |
1 Strong: AVR is indicated |
B-NR |
Symptomatic & asymptomatic patients with severe AS undergoing CABG or surgical intervention on ascending aorta. |
I: SAVR is recommended |
C |
| Apparently asymptomatic patients with severe AS & low surgical risk, when an exercise test demonstrates decreased exercise tolerance (normalized for age & sex) or a fall in SBP of ≥ 10 mm Hg from baseline to peak exercise. |
2a Moderate: AVR is reasonable |
B-NR |
Asymptomatic patients with severe AS and a sustained fall in BP (>20 mmHg) during exercise testing. |
IIa: Intervention should be considered |
C |
| Apparently asymptomatic patients with severe AS & low surgical risk, when the serum B-type natriuretic peptide (BNP) level is > 3 times normal. |
2a Moderate: AVR is reasonable |
B-NR |
Asymptomatic patients with severe AS & LVEF ≥50% if the procedural risk is low with markedly elevated BNP/NT-proBNP levels (> 3 times age- & sex-corrected normal range, confirmed on repeated measurement without other explanation). |
IIa: Intervention should be considered |
B |
| Asymptomatic patients with high-gradient severe AS & low surgical risk, when serial testing shows an increase in aortic velocity ≥ 0.3 m/s per year. |
2a Moderate: AVR is reasonable |
B-NR |
Asymptomatic patients with severe AS and LVEF ≥50% if procedural risk is low with severe valve calcification (ideally assessed by CCT) and Vmax progression ≥0.3 m/s/year. |
IIa: Intervention should be considered |
B |
| Asymptomatic patients with severe high gradient AS & a progressive decrease in LVEF on at least 3 serial imaging studies to < 60%. |
2b Weak: AVR may be considered |
B-NR |
Asymptomatic patients (confirmed by normal exercise test, if feasible) with severe, high-gradient AS & LVEF ≥50% as an alternative to close active surveillance, if procedural risk is low. |
IIa: Intervention should be considered |
A |
| Asymptomatic patients with severe AS and an LVEF < 50%. |
1 Strong: AVR is indicated |
B-NR |
Asymptomatic patients with severe AS & an LVEF < 50% without another cause. |
I: Intervention is recommended |
B |
| Asymptomatic patients with severe AS and an LVEF < 50%. |
1 Strong: AVR is indicated |
B-NR |
Asymptomatic patients with severe AS & an LVEF < 50% without another cause. | I: Intervention is recommended | B |
Asymptomatic patients with severe AS & LVEF ≥50% if procedural risk is low with LVEF <55% without another cause. |
IIa: Intervention should be considered |
B |
| Asymptomatic patients with Very severe AS (defined as an aortic velocity of ≥ 5 m/s) & low surgical risk. |
2a Moderate: AVR is reasonable |
B-R |
Asymptomatic patients with Very severe AS (mean gradient ≥60 mmHg or Vmax >5.0 m/s), LVEF ≥50%, & low surgical risk. |
IIa: Intervention should be considered |
B |
| Severe high-gradient AS & symptoms of exertional dyspnea, HF, angina, syncope, or presyncope by history or on exercise testing. |
1 Strong: AVR is indicated |
A |
Symptomatic patients with severe, high-gradient AS [mean gradient ≥40 mmHg, Vmax ≥4.0 m/s, AVA ≤1.0 cm2 (or ≤0.6 cm2/m2 BSA)]. |
I: Intervention is recommended |
B |
| Symptomatic patients with low-flow, low gradient severe AS with reduced LVEF. |
1 Strong: AVR is recommended |
B-NR |
Symptomatic patients with low-flow (SVi ≤35 mL/m2), low-gradient (<40 mmHg) AS with reduced LVEF (<50%) after careful confirmation that AS is severe. |
I: Intervention is recommended |
B |
| Symptomatic patients with low-flow, low gradient severe AS with normal LVEF, if AS is the most likely cause of symptoms. |
1 Strong: AVR is recommended |
B-NR |
Symptomatic patients with low-flow (SVi ≤35 mL/m2), low-gradient (<40 mmHg) AS with normal LVEF (≥50%) after careful confirmation that AS is severe. |
IIa: Intervention should be considered |
B |
Note: Table adapted from Otto et al., 2021 (Table 3.2.3, page e94) & Praz et al., 2025 (Table 4, page 4670).
Abbreviations: AS: Aortic stenosis; AVA: Aortic valve area; AVR: Aortic valve replacement; BNP: Brain natriuretic peptide; BSA: Body surface area; CCT: Cardiac computed tomography; COR: Class of Recommendation; LOE: Level of Evidence; LVEF: Left ventricular ejection fraction; SBP: Systolic blood pressure; SVi: Stroke volume index; Vmax: Peak transvalvular velocity
ACC/AHA 2020:
LOE A: High-quality evidence > 1 RCT, meta-analyses of RCTs, from ≥ 1 RCT corroborated by high-quality registry studies
LOE B-R: Moderate-quality evidence from ≥ 1 RCTs; Meta-analyses of moderate-quality RCTs
LOE B-NR: Moderate-quality evidence from ≥ 1 well-designed, well-executed non-randomized, observational, or registry studies
LOE C-EO: Consensus of expert opinion based on clinical experience (Meta-analyses of such studies)
COR 2a: Moderate, Is reasonable, Can be useful/effective/beneficial (Benefit >> Risk)
ESC/EACTS 2025:
LOE A: Data derived from multiple randomized clinical trials or meta-analyses
LOE B: Data derived from a single randomized clinical trial or large non-randomized studies
LOE C: Consensus of opinion of the experts and/or small studies, retrospective studies, registries
Table 7. ACC/AHA 2020 & ESC/EACTS 2025 clinical guideline recommendations for mode of intervention (TAVR; SAVR) in AS patients
| ACC/AHA 2020 |
ESC/EACTS 2025 |
| Patient Assessment |
COR |
LOE |
Patient Assessment |
COR |
LOE |
| Symptomatic and asymptomatic patients with severe AS and any indication for AVR who are < 65 years of age or have a life expectancy >20 years. |
1 Strong:SAVR |
A |
Patients < 70 years of age, if the surgical risk is low |
I: SAVR |
B |
| Symptomatic patients with severe AS who are 65 to 80 years of age and have no anatomic contraindication to transfemoral TAVR. * Choice of TAVR vs SAVR should be made after shared decision making about the balance between expected patient longevity and valve durability. |
1 Strong: Either SAVR or transfemoral TAVR * |
A |
All remaining candidates for an aortic BHV according to Heart Team assessment |
I: SAVR or TAVI |
B |
| Symptomatic patients with severe AS who are >80 years of age or for younger patients with a life expectancy <10 years and no anatomic contraindication to transfemoral TAVR. |
1 Strong: Transfemoral TAVR |
A |
Patients ≥ 70 years of age with tricuspid AV stenosis, if the anatomy is suitable |
I: TAVI |
A |
| Asymptomatic patients with severe AS and an LVEF <50% who are ≤ 80 years of age and have no anatomic contraindication to transfemoral TAVR. |
1 Strong: Follow the same recommendations as for symptomatic patients in the 3 recommendations listed in the above rows. |
B-NR |
|
| Asymptomatic patients with severe AS, an abnormal exercise test, very severe AS, rapid progression, or an elevated BNP (COR 2a indications for AVR). |
1 Strong: SAVR |
B-NR |
|
| Patients with an indication for AVR for whom a bioprosthetic valve is preferred but valve or vascular anatomy or other factors are not suitable for transfemoral TAVR. |
1 Strong: SAVR (Benefit >>> Risk) |
A |
|
| Symptomatic patients of any age with severe AS and a high or prohibitive surgical risk. ** If predicted post-TAVR survival is >12 months with an acceptable quality of life. |
1 Strong: TAVR ** |
A |
|
Note: Table adapted from Otto et al., 2021 (Table 3.2.4.2, page e55-56) & Praz et al., 2025 (Table 4, page 4670).
Table 8. Summary of factors favoring TAVR (versus SAVR or clinical surveillance) for the treatment of severe AS patients
| ACC/AHA 2020 (Otto et al., 2021) |
ESC/EACTS 2025 (Praz et al., 2025) |
| Older age, with fewer expected years remaining. TAVR is recommended over SAVR in patients aged > 80 years or in younger patients with a life expectancy < 10 years and no anatomic contraindication to transfemoral TAVR. |
≥ 70 years |
| Recommended for patients with symptomatic severe AS aged 65 to 80 years (and no anatomic contraindication to transfemoral TAVR) after shared decision-making about balance between expected patient longevity and valve durability. SAVR may also be offered to these patients. |
Transfemoral access suitable for TAVI. |
| In asymptomatic patients with severe AS and an LVEF < 50% who are ≤ 80 years of age and have no anatomic contraindication to transfemoral TAVR, the decision between TAVR and SAVR should follow the same recommendations as for symptomatic patients. |
|
| For symptomatic patients of any age with severe AS and a high or prohibitive surgical risk, TAVR is recommended if predicted post-TAVR survival is > 12 months with an acceptable quality of life. |
|
| When TAVR risk is low to medium; SAVR risk is high to prohibitive. |
|
| In patients with a calcific AS of a trileaflet valve. |
|
| When a bioprosthetic (versus mechanical) valve is preferred. |
|
| In patients who have a favorable ratio of life expectancy to valve durability. |
|
| In patients who have a severe calcification of the ascending aorta (“porcelain” aorta), severe lung, liver, or renal disease, mobility issues (high procedural risk with sternotomy), with frailty that is likely to improve after TAVR, with previous cardiac surgery and at-risk coronary grafts, or in patients with previous chest irradiation. |
Porcelain aorta, intact coronary artery bypass grafts, severe chest deformity or scoliosis, comorbidities or cardiac conditions increasing surgical risk, frailty, sequelae of chest radiation. |
| If the goals of care and patient preferences are a shorter hospital stay, and less post-procedural pain and they accept the uncertainty about valve durability and possible repeat intervention. |
|
1 This “availability of TAVR” included thorough preparation for the TAVR procedure for each patient in advance; patients in the surveillance arm were told they would (eventually) get this life-saving treatment when symptoms developed, and then both patients and physicians waited for those symptoms to occur. It is not surprising that symptoms did occur, and quickly, leading some experts to refer to this as a “self-fulfilling” trial design.


