Integrated Care for Kids (InCK) Model
Overview
The Center for Medicare and Medicaid Innovation (Innovation Center) has announced a new model, tested under the authority of section 1115A of the Social Security Act, as part of a multi-pronged strategy to combat the nation’s opioid crisis. The Integrated Care for Kids (InCK) Model is a child-centered local service delivery and state payment model aimed at reducing expenditures and improving the quality of care for children covered by Medicaid and the Children’s Health Insurance Program (CHIP) through prevention, early identification, and treatment of priority health concerns like behavioral health challenges and physical health needs. The model will offer states and local providers support to address these priorities through a framework of child-centered care integration across behavioral, physical, and other child providers.
Why develop a model for children?
Behavioral health conditions in children and youth, including use of opiates and other substances, drive significant morbidity, health care utilization, and premature death. One in three children in Medicaid and CHIP have behavioral health needs, yet only one-third of those in need receive care.[1] Furthermore, adolescent deaths from drug overdose are increasing, and opioids caused over half of drug-related overdoses among youth in 2015.[2]
The current child health care system has challenges in identifying and addressing risk factors for behavioral health conditions, because the earliest signs of a problem may present outside of clinical care—such as behavioral problems in schools, or chaotic family situations known to child welfare and foster care programs. Although a variety of federal, state, and local services exist to support children’s health, limited information sharing and differing eligibility and enrollment processes may create barriers to putting children and families at the center of their care.
The goals of the InCK Model are to improve child health, reduce avoidable inpatient stays and out of home placement, and create sustainable alternative payment models (APMs)[3]. The InCK Model will support states and local providers to conduct early identification and treatment of children with health-related needs across settings. Participants will be required to integrate care coordination and case management across physical and behavioral health and other local service providers to provide child- and family-centered care. Finally, through the APM that is developed through this model, states and local providers will share accountability for cost and outcomes. These interventions are designed to increase behavioral health access, respond to the opioid epidemic and positively impact the health of the next generation.
What are the model’s goals?
The InCK Model will award states and local communities cooperative agreements to build on existing delivery system innovations with the goals of:

How will the model achieve these goals?
The InCK Model aims to achieve these goals through:

InCK participants will deliver child- and family-centered integrated care and case management for children with physical, behavioral, and other health-related needs like food insecurity and unstable housing. Model participants will build community capacity to provide more effective, efficient, and affordable care through home- and community-based services (HCBS), reducing unnecessary inpatient stays and out-of-home placements. State participants will work with CMS and Lead Organization to develop APMs responsive to local contexts and priorities that leverage the broad array of existing mandatory and optional Medicaid and CHIP benefits to empower providers and promote cost-savings, improved quality, and state flexibility.
Who will participate in the model?
The key participants of the InCK Model will be the state Medicaid agency and a local entity called a “Lead Organization.”
 |

|

|
| Lead Organizations will convene community partners to integrate coordination and management of the InCK Model’s core child services for the attributed population. The Lead Organization will be accountable for improving population-level care quality and outcomes and developing service integration protocols and processes. HIPAA-covered entities, including state Medicaid agencies, will be eligible to serve as Lead Organizations. | State Medicaid Agencies will support local implementation by providing population-level data for the geographic service area, supporting the development of information sharing arrangements and infrastructure, working to align support for the model across child-focused state agencies, and developing the pediatric APM. State Medicaid agencies will participate in the model regardless of whether they also serve as the Lead Organization. |
CMS will award up to 8 states. Either a State Medicaid Agency or a Lead Organization will be the awardee of a cooperative agreement.
Whom will the model serve?
InCK Model participants must be prepared to serve all children covered by Medicaid and CHIP, if applicable, from the prenatal period up to 21 years of age residing within an awardee-specified (and CMS-approved), sub-state geographic service area.
What are key design elements of the model?
Core Child Services
Lead Organizations will coordinate the integration of the following core child service types. Lead Organizations may consider including other child service types as appropriate.

Service Integration
The InCK Model offers Lead Organizations and their partners the flexibility to employ service integration strategies most appropriate for achieving the model’s aims in their local context.
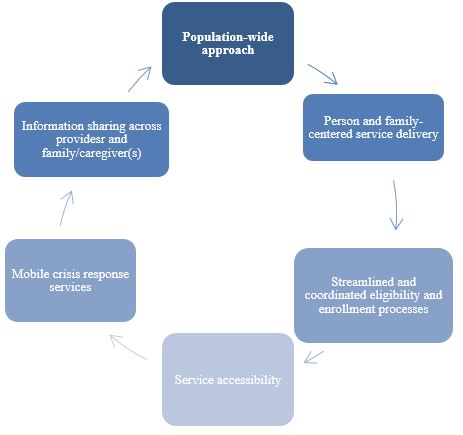
The six key service integration design characteristics that awardees must incorporate in their implementation plan are:
Risk Stratification Approach and Tiered Service Delivery
The InCK service integration structure is based on population-wide risk-stratification according to level of need. Service Integration Levels (SILs) consist of integrated care coordination and case management levels of increasing intensity appropriate for individual needs. The goal of stratification is to ensure that children receive the individualized care they need in the most integrated and least restrictive setting appropriate.
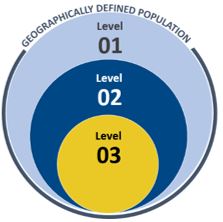
SIL 1 includes all children covered by Medicaid or CHIP up to age 21 residing in the awardee’s geographic service area. Children in SILs 2 and 3 have multi-sector needs, functional impairments, and are at-risk for or currently placed outside of their home.
Alternative Payment Models
States will work with CMS and the Lead Organization to design and implement one or more child-focused APMs in Medicaid (and CHIP, if applicable). States with existing APMs may instead alter as necessary to meet the model’s criteria. The model will require participating states to develop APMs for supporting care coordination, case management, and mobile crisis response and stabilization services via existing authorities available under Medicaid and CHIP. The goals of the APMs are to 1) promote accountability for improved outcomes, such as rates of avoidable out-of-home placement and opiate use, and 2) ensure the model’s sustainability long-term.
How will funding be awarded?
InCK Model funding will be awarded via cooperative agreement. CMS has released a Notice of Funding Opportunity (NOFO) to solicit applications for up to eight cooperative agreements under the InCK model. Each cooperative agreement will be up to $16 million for the seven-year model period. Applicants will need to explain how they will use existing funding sources to deliver services to beneficiaries because model funding may be used only to support model planning and implementation activities. The state Medicaid agency and Lead Organization will partner together to write the application, but only one of these entities will be considered the applicant and the model awardee. The NOFO explains additional model and application requirements, as well as awardee eligibility criteria.
Applications are due by 3pm ET to Grants.gov on June 10, 2019.
What is the model timeline?
The Integrated Care for Kids Model is expected to begin in early 2020 with a two-year pre-implementation period in which CMS will work with states and Lead Organizations to assist the states in establishing or modifying any needed Medicaid and CHIP authorities and provide technical assistance to develop the infrastructure and procedures necessary for model implementation. A five-year model implementation period will follow in which states and Lead Organizations will implement their  models and report required data to CMS.
models and report required data to CMS.
Email: HealthyChildrenandYouth@cms.hhs.gov
Visit: https://innovation.cms.gov/initiatives/integrated-care-for-kids-model/
###
Get CMS news at cms.gov/newsroom, sign up for CMS news via email and follow CMS on Twitter CMS Administrator @SeemaCMS, @CMSgov, and @CMSgovPress.
[1] Department of Health and Human Services, 2016. 2015 Annual Report on the Quality of Care for Children in Medicaid and CHIP.
[2] Department of Health and Human Services, 2017. Office of Adolescent Health “Opioids and Adolescents”. Retrieved from: https://www.hhs.gov/ash/oah/adolescent-development/substance-use/drugs/opioids/index.html.
[3] Alternative payment models for the purposes of the InCK Model are not Alternative Payment Models as defined at 42 CFR §1305 for the purpose of the Quality Payment Program, which are defined as: (1) A model under section 1115A of the Act (other than a health care innovation award); (2) The Shared Savings Program under section 1899 of the Act; (3) A demonstration under section 1866C of the Act; (4) A demonstration required by Federal law.